Download
1 / 46
630 likes | 1.94k Views
MITRAL STENOSIS . Nick Tehrani, MD. Epidemiology of MS. Hx of Rheumatic fever is elicited in only 50% of path proven cases Other causes Severe MAC Congenital MS. Clinical Diagnosis of Rheumatic Fever. Diagnosis of acute rheumatic fever Two major Jones criteria, OR

E N D
MITRAL STENOSIS Nick Tehrani, MD
Epidemiology of MS • Hx of Rheumatic fever is elicited in only 50% of path proven cases • Other causes • Severe MAC • Congenital MS
Clinical Diagnosis of Rheumatic Fever • Diagnosis of acute rheumatic fever • Two major Jones criteria, OR • One major criterion, and two minor criteria MajorMinor Carditis Fever Erythema marginatum PR prolongation Chorea ESR elevation Subcutaneous nodules Hx of Rheumatic fever
Clinical Diagnosis of Acute Rheumatic Fever • Additionally, serologic evidence of recent streptococcal infection is needed: • Positive bacteriologic culture • Increase in ASO titers • Increase in anti-DNAse B titers
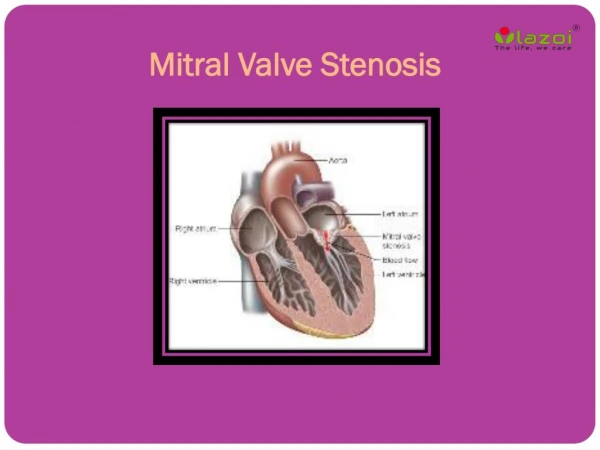
Histopathology • The acute valvular pathology caused by Rheumatic fever is: Mitral Regurgitation • Over the next several decades stenosis accrues by: • Thickening of the leaflets • Fusion of the commisures • Fusion or shortening of the chordae
Definitions of severity of Mitral Stenosis • Valve Area: • <1.0 cm2 Severe • 1.0-1.5 cm2 Moderate • >1.5-2.5 cm2 Mild • Mean gradient: • >10 mmHg Severe • 5-10 mmHg Moderate • <5 mmHg Mild
Flow Across the Stenotic Valve • Persistent LA-LV gradient in diastole sustained flow throughout diastole • The slope of the envelope is proportional to the severity of stenosis
Flow Across the Stenotic Valve • Note the “A” in patient who is in sinus
Diastolic Transmitral Pressure Gradient due to Limited LV Filling
Pathophysiology • Limited flow into the LV has 3 major sequale: • Elevation of Lt. Atrial pressure • Secondary RV pressure overload • Reduced LV ejection performance • Due to diminished preload • Tachycardic response to compensate to decreased SV worsens the transmitral gradient
Determinants of Transmitral Pressure Gradient Increased Flow, OR Decreased orifice size Incr. Gradient. Elevated LA pressure
HR=72 HR=100
Variability Problems are Introduced by: • The three inter-related parameters are: • HR • CO • Trans-mitral gradient Mitral valve area Heart rate variability CO measurement and reproducibility
Different ways of Measuring Mitral Valve Area • Echocardiographic: • PISA • 2-D • Pressure half-time • Cath: • Gorlin’s Equation • Pressure half time
The Gorlin Equation • Torricelli’s Law: • Cc =Coefficient of • Orifice contraction • The Second Equation: • Cv=Coefficient of • Velocity
The Gorlin Equation • Substituting for V, in Torricelli’s Eq. C 44.3 Simplification of the above: ?
The Numerator of the Equation • Flow Across any Valve: • For Mitral (and Tricuspid) valve:
The Gorlin Equation • Substituting for “Flow” and “h” in the first Eq.:
Gorlin’s Formula for Mitral Area • The Gorlin Formula for Mitral Valve area:
Gorlin’s Formula for Mitral Area • CO Cardiac output • DFP Diastolic Filling Period • HR Heart Rate • 44.3 Derived Constant • C Correction factor for valve type C=1.0 for all valves except Mitral C=0.85 for Mitral valve • P Mean pressure gradient
Step 1: Figure out the Numerator First: Dimensional analysis: How Do you use this Eqn.?
DFP in Sec/beat Measure the Distance in mm from MV opening to MV closing in one beat Convert distance to time 100 speed= 100 mm/sec, makes life easy 50 speed= 50 mm/sec, tough life Figure out the DFP
Assuming Patient is in Sinus Measure the RR interval in mm Convert to Beats/min by… In 100 speed just divide 6,000 by the RR in mm Figure out the Heart Rate
Diastolic Transmitral Pressure Gradient due to Limited LV Filling Left Atrial Tracing
C A V Planimeter DFP Shifted Over
Instrumentation • The trickiest part is to set up the instrument correctly: • The reading must be adjusted to • 0.0000
From Planimetered Area to Mean Pressure Gradient • Area as provided by the instrument is in (in)x(in) • Must convert to (cm)x(cm) • Multiply by 6.45 cm2/In2 • To obtain mean Area under the curve • Divide the Area by the DFP in cm • To convert cm of pressure to mm of Hg • Multiply the above # in cm, by the “scale factor” • Get “Scale factor” from the tracing: mm Hg/cm
How many tracings to Planimeter • If patient is in sinus => 5 tracings • If patient is in A-Fib.=> 10 tracings
Putting things in Perspective CC/Sec cm2 CC/sec.cm2.(mm Hg)P0.5 mm Hg
Potential Pitfalls • Wedge vs. LA Pressure • Stiff End-hole catheter: Cournand • Verify true wedge by checking O2 Sat • Mean Wedge should be less than Mean PA • Cardiac Output • True Fick vs. Thermodilution vs. Green dye • Concurrent MR with MS: • Gradient across the valve reflects forward and regurgitant flow • CO reflects the net forward flow only • Likely underestimation of the true valve area
Mitral Stenosis and the LA • Even in sinus rhythm, the low velocity flow predisposes to formation of atrial thrombi. • Low flow pattern is seen as spontaneous contrast on echocardiography • 17% of patients undergoing surgery for MS have LA thrombus • In one third of cases thrombus restricted to the LAA
Pulmonary Hypertension • Normal pressure drop across pulmonary bed: 10-15 mm Hg • Expected mean PA in Mitral Stenosis: Mean LA (elevated of course) + (10-15 mm Hg) • In MS, Mean PA pressure often exceed the expected.
Pulmonary Hypertension • This pulmonary hypertension has two components: • Reactive pulmonary arterial vasoconstriction, • Potentially Fixed resistance, secondary to morphologic changes in the pulmonary vasculature
Step 1: Figure out the Numerator First: Dimensional analysis: How Do you use this Eqn.?
DFP in Sec/beat Measure the Distance in mm from MV opening to MV closing in one beat Convert distance to time 100 speed= 100 mm/sec, makes life easy 50 speed= 50 mm/sec, tough life Figure out the DFP
Assuming Patient is in Sinus Measure the RR interval in mm Convert to Beats/min by… In 100 speed just divide 60,000 by the RR in mm Figure out the Heart Rate
C A V Planimeter DFP
From Planimetered Area to Mean Pressure Gradient • Area as provided by the instrument is in (in)x(in) • Must convert to (cm)x(cm) • Multiply by 6.45 cm2/In2 • To obtain mean Area under the curve • Divide the Area by the DFP in cm • To convert cm of pressure to mm of Hg • Multiply the above # in cm, by the “scale factor” • Get “Scale factor” from the tracing: mm Hg/cm