Download
1 / 22
220 likes | 389 Views
HIV Disease and Complications of Immunodeficiency. Chapter 29. HIV Disease. Symptoms Appear after incubation period of 6 days to 6 weeks Usually consist of fever, headache, sore throat, muscle aches, enlarged lymph nodes and generalized rash Some develop CNS symptoms

E N D
HIV Disease and Complications of Immunodeficiency • Chapter 29
HIV Disease • Symptoms • Appear after incubation period of 6 days to 6 weeks • Usually consist of fever, headache, sore throat, muscle aches, enlarged lymph nodes and generalized rash • Some develop CNS symptoms • Range from moodiness and to seizures and paralysis • Symptoms constitute acute retroviral syndrome (ARS) • Typically subside in 6 weeks • Acute illness followed by asymptomatic period • Period may end with persistent enlargement of lymph nodes • Lymphadenopathy syndrome (LAS) • Immunodeficiency symptoms include fever, weight loss, fatigue and diarrhea • Referred to as AIDS-related complex (ARC)
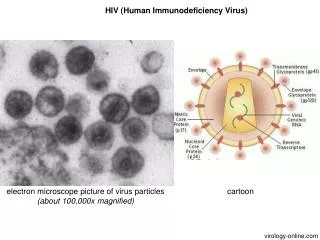
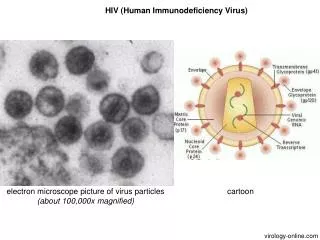
HIV Disease • Causative agent • In U.S and most other parts of the world disease caused by human immunodeficiency virus type 1 (HIV-1) • Belongs to lentivirus subgroup of retrovirus family • HIV-2 is similar in structure to HIV-1 but is antigenically distinct • Prominent cause of AIDS in parts of West Africa and India • Has appeared in the U.S. • Transmission is less efficient than HIV-1 • Disease progresses slower
HIV Disease • Pathogenesis • HIV attacks a variety of cell types • Most critical are helper T cells • Viral gp120 attaches to CD4 cell surface receptor • Viral gp41 induces membrane fusion by interacting with chemokine cell surface receptor (CCR) • After entry, DNA copies of RNA genome produced using reverse transcriptase viral enzyme • DNA copy integrates and hides on host chromosome • In activated cells virus leaves cell genome and kills cell • Releases additional viruses to infect other cells • Macrophages have CD4 receptors • Infected macrophages are not killed but are impaired • Eventually immune system becomes too impaired to respond
HIV Disease • Pathogenesis • Destruction of immune system helper T cells by HIV can occur via multiple mechanisms • Lysis following HIV replication • Attack by HIV-specific cytotoxic CD8+ T lymphocytes • CTL kill HIV-infected T cells • Antibody-dependent cellular cytotoxicity • Antibodies bind to gp120 and gp41 viral glycoproteins on infected T cells, facilitating the killing of those cells • Autoimmune process • Fusion of infected and uninfected cells • Facilitated by gp120 and gp41 on infected cells and CD4 and CCR on uninfected cells • Apoptosis • Accelerated in HIV infections
HIV Disease • Pathogenesis • In nearly 80% of all cases immune system slowly loses ground to virus • Peripheral CD4+ count steadily falls to nearly 50 cell /µl • Symptoms usually appear when count falls below 200 cells/µl • Atypical progression of disease occurs in roughly 10% of infected individuals • Disease progresses rapidly to AIDS within a few months • Another 5% - 10% do not experience a fall in CD4+ cells • Maintain high levels of antibodies and CD8+ cells • Disease progresses slowly • May be AIDS-free for 20 years
HIV Disease • Epidemiology • Indiscriminate sexual intercourse major factor in spread • Promiscuous homosexual men most common • Survey indicates before arrival of AIDS 33% to 40% of homosexual men had more than 500 lifetime partners • Next most important mode of transmission is through blood and blood products • By 1984 over 50% of hemophiliacs in U.S. were infected • 10% - 20% of their sexual partners were HIV positive • Today, blood transmission is usually I.V. drug use (needle-sharing) • Third most important mode of transmission is mother to infant • One in 10 pregnant HIV-positive women will miscarry • Of live-born infants, 15% - 40% will develop AIDS • Breast feeding carries significant risk of mother-infant transmission
HIV Disease • Prevention and Treatment • No approved vaccine • Most people infected are unaware • Virus on surfaces can be inactivated with commercially available disinfectants and heat at 56°C for more that 30 minutes • Knowledge of transmission greatest tool for control • Use of condoms not 100% effective but have been shown to decrease transmission • Avoidance of practices that favor HIV transmission
HIV Disease • Prevention and Treatment • Treatment directed at “cocktails” of drugs • Combination of reverse transcriptase inhibitors and protease inhibitors • HAART = highly active antiretroviral therapy • Reverse transcriptase inhibitors fall into two categories • Nucleoside reverse transcriptase inhibitors • Zidovudine (AZT), stavudine (D4T) and lamivudine (3TC) • Non-nucleoside reverse transcriptase inhibitors • Nevirapine, efavirenz and delavirdine
HIV Disease • Prevention and Treatment • Highly-Active Anti-Retroviral Therapy • Protease inhibitors • 6 in use • Act late in HIV replication to prevent packaging of viral proteins • HAART does not cure AIDS • Viremia becomes undetectable in approximately 50% of cases • Will reappear in absence of treatment • Many strains fail to respond to HAART due to resistance
HIV Disease • HIV vaccine prospects • Currently no approved vaccines • In theory, vaccine could be used in two ways • Prevention vaccine • Immunize uninfected individuals against disease • Therapeutic vaccine • Boost immunity of those already infected • Successful vaccine must • produce both mucosal and blood stream immunity • get around HIV variability and stimulate cellular and humoral immunity
HIV Disease • HIV vaccine prospects • Attenuated agent must not: • Be capable of turning into disease-causing strain • Be oncogenic • Stimulate an autoimmune response • Cause production of “enhancing” antibodies that could aid in the passage of HIV into the body’s cells • Finally, vaccine should induce neutralizing antibodies against free virions and prevent direct spread of HIV from cell to cell • Vaccine trial in humans has been undertaken for at least 10 experimental vaccines • All have failed and prospects do not look favorable
Kaposi’s Sarcoma • Unusual tumor arising from blood or lymphatic vessels in multiple locations • Common in men of Mediterranean and Eastern European descent • Not as a sign of immunodeficiency • Tumor began to appear in young men with HIV • 2000 time higher than period before HIV • So common among AIDS patients became AIDS-defining condition
Kaposi’s Sarcoma • Human herpesvirus-8 (HHV-8) detected in sarcomas • Virus infects endothelial cells that line blood and lymphatic vessels • Persists mostly in latent form • Presence of virus associate with two dramatic changes that result in tumor formation: • Cells assume spindle shape and proliferate • Extensive formation of new blood vessels occurs
B-Lymphocytic Tumors of the Brain • B-cell lymphomas 60 to 100 times more common in AIDS patients compared to general public • Intense, sustained replication of lymphoid cells is constant feature of HIV • Lymph node enlargement reflects proliferation of lymphoid cells in response to high level unregulated cytokine release • Replication of T cells occurs to replace those destroyed by HIV • Epstein-Barr virus plays roll in B-cell lymphomas associated with AIDS • Lymphomas rarely occur in brain except with AIDS patients
Pneumocystosis • Symptoms • Typically begins slowly with gradually increasing shortness of breath and rapid breathing • Fever is usually slight or absent • 50% of patients have non-productive cough • Skin and mucous membranes becomes dusky • Due to poor oxygenation of blood
Pneumocystosis • Causative agent - Pneumocystis carinii • Tiny fungus belonging to phylum Ascomycota • Formerly considered a protozoan • Differs from many fungi in cell wall components • Consequently resistant to many fungal medications • Pathogenesis • Spores of organism are inhaled into lung • Attach to alveolar walls • Alveoli fill with fluid, mononuclear cells and organisms • Alveolar walls become thickened and scarred • Interferes with free passage of oxygen
Pneumocystosis • Epidemiology • Widespread among animals including dogs, cats, horses and rodents • Serological testing indicates almost all children are infected by age two and a half • Infection is asymptomatic and generally eliminated in a year • Source of transmission in humans is unknown • Most cases of pneumocystosis occur in immunocompromised • Epidemics among hospitalized malnourished infants and elderly nursing home residents suggest airborne spread
Pneumocystosis • Prevention and Treatment • Disease used to occur in four-fifths of AIDS patients • Was leading cause of death • Disease largely preventable with regular doses of trimethoprim-sulfamethoxazole (TxS) • Among the best medication for treating disease along with oxygen support • Reduced mortality rate from nearly 100% to 30% • After treatment patient must receive preventive medication indefinitely until rise in CD4+ T cells above 200 cells/μl
Other Common Opportunistic Infections of AIDS • Toxoplasmosis (Toxoplasma gondii) • Herpesviruses • Herpes simplex viruses 1&2 • Cytomegalovirus • Mycobacterium avis (TB-like disease)