Download
1 / 29
290 likes | 405 Views
See agenda for April 20 th on slide 3. Care Plan (CP) Team Meeting Notes (As updated during meeting). André Boudreau (a.boudreau@boroan.ca) Laura Heermann Langford (Laura.Heermann@imail.org) 2011-04-13 (No. 9). HL7 Patient Care Work Group. Agenda for April 13th.

E N D
See agenda for April 20th on slide 3. Care Plan (CP) Team Meeting Notes(As updated during meeting) André Boudreau (a.boudreau@boroan.ca) Laura Heermann Langford (Laura.Heermann@imail.org) 2011-04-13 (No. 9) HL7 Patient Care Work Group
Agenda for April 13th • Email notes from Kevin, Lloyd, William, Cecil • Storyboard criteria (Laura, Stephen, Danny) • Introduction to Eclipse Workbench (Kevin): download and quick start • Updated high level processes (Stephen) • Issue: overarching term: condition, concern, problem?
Agenda for April 20 • Care Plan elements from KP, Intermountain, etc. (Laura) • Feedback on models prepared by Stephen (Laura and Susan) • Updated doc on storyboards (Danny) • IHE Patient Plan of Care (PPOC) (Ian) • Modeling tool to use (Eclipse or EA) (André) • Overarching term to use (Ian M.) • Business requirements: summary of key aspects since February (André) • This will become eventually our first formal deliverable • Next meeting agenda
Notes sent by email- 2011-04-06 • Kevin Coonan • (1) The medication list is defined by the care plan. It is part of the therapy for a given problem. • (2) The "problem list" is largely covered as well by the care plan. If you are getting a specific therapy or plan for something, it is a problem (health concern!). • (3) We really need to determine which file formats are allowed. There are a lot of tools, many of which overlap in what software can use it, so we should be able to settle on some parsimonious set (mind map, outline, text files, information models, UML, etc.). • Lloyd McKenzie: • Usually "Medication List" refers to what meds a patient is on, not what the care plan intends them to be on. The lists are often quite different. You may or may not have a care plan for a given problem. But a patient's current problem list would be of interest for all care plans. Use these notes where applicable in our work.
Email 1 from William 2011-04-07 • We have a hierarchy established and reconfirmed many times • Guideline is the upper level framework • Which can be expressed as critical pathway • Which can be expressed in a care plan (Using the Care Plan R-MIM in Care Provision) for which we are now creating the DAM. • Which can have order sets (e.g. a section taken from the guideline and expressed as part of a care plan, e.g. a discharge planning set of activities). • Which can have any kind of list (e.g. using the Care Provision Statement Collector 1 to many times, e.g. one statement collector for observation list, one SC for problem list, one for medication list, one for action plan, one for outcome indicators, one for the discharge planning etc. Each SC can get a meaningful name. This way the Care Plan R-MIM can on runtime have 100 Statement Collectors, each containing a million clinical statements….! • Many manymany individual care statements / clinical statements. Which is the bottom of the hierarchy • Each Care Provision message can hold one or more of the above constructs 1-6. A Care Provision message can have one clinical statement, or can have 7657543 clinical statements, ordered with the above hierarchy, or as a flat series. Because most clinicians want some order we have the organizer to link some clinical statements that belong together, the statement collector to group a series of similar clinical statements and the care plan for obvious reasons to reflect practice. The guideline is more the input of knowledge to this. • Response from Cecil Lynch • This is not a taxonomic hierarchy but rather relationships among artifacts. Please evaluate each of these levels as an IS A statement and that will help you establish a hierarchy that is accurate. First 3 bullets not HL7 specific. Pathway is organizational specific.
Email 2 from William 2011-04-07 • This is part of the current Normative Edition, in particular the R-MIMs and D-MIM I refer to and their explanation. • The order I suggested is not really a taxonomy as Cecil suggests, it is not completely representable in a ‘IsA’ relationship approach, it just a matter of organizing it in our heads as what is available and how is it related to each other. That part of organizing it has been discussed on several O&O and CDS and PC joint meetings of the past 3-4 years. Always on Monday Q4 meetings, where O&O has the minutes. I agree it needs to be documented and the wiki is a much better place for this. Let me do that during the WGM CP meeting. I will be there and listen. • Care Statements can be organized according to the Organizer Class, according to Statement Collector(s), according to Care Plan so that is a bottom up relationship. • Top down it can be as: • Organizer class is a collection of 1-n different clinical statements that are usually grouped together. • Assessment scale representation is a specific organizer of clinical statements that are collected and exchanged together because they are stated on the same date / time. • Statement collector is a collection of 1-n the same or similar clinical statements that are usually stated on different dates and times • Care Care plan is a collection of several organizer classes representing 1-n clinical statements and / or a collection of statement collectors, and/or a collection of individual clinical statements and or other organizations of clinical statements (that is part of our current DAM work, to explore other means). • Care Record R-MIM is a collection of clinical statements and/or a collection of clinical statements, such as organized care statements, care statements in statement collector(s), and/or care plan(s), and/or other collections further expressed in the R-MIM collection of the domain. Use these notes where applicable in our work.
Storyboard criteria • See Danny’s document as annotated during the discussion • See next slide with Stephen’s input • Need to align with HDF 1.5 as this was decided in a previous meetings • See pages 27-28 and Appendix 1 of Power Point deck of 2011-03-02 meeting • Danny will update his document and resubmit for discussion • Post meeting comment by André: suggest that the above document be restricted to Storyboards for now, since we already have the HDF 1.5 methodology document plus another document listing our deliverables for this phase
Storyboard: what is it? Narrative of business (clinical; administrative) processes on domain/area of interest Non technical (conceptual in nature) Describes: Activities, interactions, workflows Participants High level data contents feeding into or resulting from processes Provides inputs for: Activity diagrams Interaction diagrams State transition diagrams High level class diagrams Stephen Chu 12 April 2011
Care Plan Elements from KP, Intermountain, etc. • Request wss sent out by Laura • Some initial feedback, better to wait next week
Introduction to Eclipse Workbench • We need to agree on a tool to do: • Use cases • Activity and workflow diagrams • Interaction diagrams • Class models • Eclipse is a platform for doing many different things using specific plug-ins • Recommended by HL7 • Open Source but not as intuitive as Enterprise Architect (which costs some 100$ for a desktop version) • Ask publishing committee • If Eclipse, we need some coaching to download and quick start Eclipse • Add plug-in for UML • Adel agreed to help us there
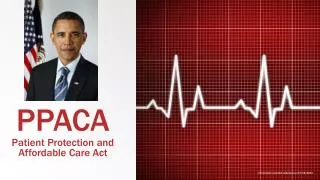
Care Plan – High Level Processes Initial Assessment Identify problems/issues/reasons Assess impact/severity: referral order tests Determine Problems & Outcomes Confirm/finalize problem/issue/reason list Determine goals/intended outcomes Determine/plan appropriate interventions Develop Plan of Care Set outcome target date Determine/assign resources healthcare providers other resources Care Plan Implementation Implement interventions Follow-up Actions Evaluate patient outcome Evaluation Document outcomes Review interventions Revise/modify interventions OR Close problem/issues/reason/care plan From April 6th Goals/Outcomes: - Optimize function - prevent/treat symptoms - improve functional capability - improve quality of life - Prevent deterioration - prevent exacerbation; and/or - prevent complications - Manage acute exacerbations - Support self management/care This is based on a broad review. All converge. Need a concept of a master care plan with all the concerns and problems May need to revise goals and outcomes during the process of care. Nutrition has similar model. Also use standardized language Hierarchy or interconnected plans can apply. Every prof group has specific ways to deliver care. Here we focus on the overall coordination of care. Is there always a care coordinator? Patients could be the coordinator of their own care. They should be active participants. This diagram is about process, not Interactions and actors Add care coordination activities in these activities Care Plan Stephen Chu 5 April 2011
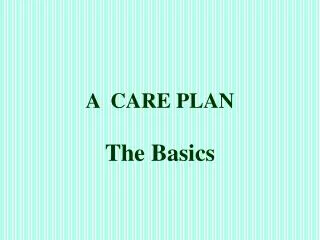
Care Plan – High Level Processes IHE has more loose connections. Here assumes workflow engine that connects tightly problem, goal, task. Need distinct process to manage/communicate/update/track/close the Care Plan. See IHE. Make more explicit here. High Level Shared Plan Initial Assessment Problem/concern/reason 1..* Target goals/outcomes Planned intervention Assessed outcome Identify problems/issues/reasons Assess impact/severity: referral order tests Confirm/finalize problem/concern/reason list Determine goals/intended outcomes Develop Plan of Care Detailed Care Plan Determine/plan appropriate interventions Refer to other provider (s) Set outcome target date Determine/assign resources healthcare providers other resources Care Plan Implementation Implement interventions Follow-up Actions Evaluate patient outcome Evaluation Document outcomes Review interventions Revise/modify interventions OR Close problem/issues/reason/care plan April 13 This is illustrative Goals/Outcomes: - Optimize function - prevent/treat symptoms - improve functional capability - improve quality of life - Prevent deterioration - prevent exacerbation; and/or - prevent complications - Manage acute exacerbations - Support self management/care Care orchestration Determine Problems & Outcomes Care orchestration Care Plan Need to study this more: Laura and Susan to work on it Stephen Chu 12 April 2011
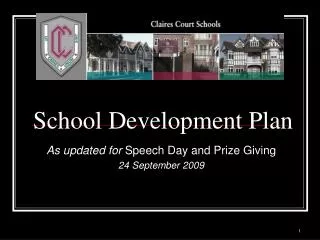
Care Plan – Process-based Structure Initial Assessment Diagnosis/problem/issue - primary - secondary … Identify problems/issues/reasons Assess impact/severity: referral order tests Problem/issue/risk/reason Desired goal/outcome Outcome target date Determine Problems & Outcomes Confirm/finalize problem/issue/reason list Determine goals/intended outcomes Planned intervention/care service Planned intervention datetime/time interval (including referrals) links to other care plan as service plan Responsible healthcare & other provider(s) Determine/plan appropriate interventions Develop Plan of Care Set outcome target date Determine/assign resources healthcare providers other resources Intervention review datetime Responsible review party/parties Care Plan Implementation Implement interventions Follow-up Actions Evaluate patient outcome Evaluation Review outcome Document outcomes Review interventions Review recommendation/decision Revise/modify interventions OR Close problem/issues/reason/care plan Need to decide what tool to use for the next version From April 6th Goals/Outcomes: - Optimize function - prevent/treat symptoms - improve functional capability - improve quality of life - Prevent deterioration - prevent exacerbation and/or - prevent complications - Manage acute exacerbations - Support self management/care Need a master plan with linkages to sub-plans Same as the problem list 2 levels: global that everyone Can see: what by whom. Then a detail Care Plan Stephen Chu 5 April 2011
Care Plan – Process-based Structure Will need to add explanations and maybe some different scenarios High Level Shared Plan Initial Assessment Problem/concern/reason 1..* Target goals/outcomes Planned intervention Assessed outcome Identify problems/issues/reasons Assess impact/severity: referral order tests Determine Problems & Outcomes Problem/issue/risk/reason Desired goal/outcome Outcome target date Confirm/finalize problem/concern/reason list Determine goals/intended outcomes Develop Plan of Care Planned intervention/care service Planned intervention datetime/time interval (including referrals) links to other care plan as service plan Responsible healthcare & other provider(s) Determine/plan appropriate interventions Refer to other provider (s) Set outcome target date Determine/assign resources healthcare providers other resources Intervention review datetime Responsible review party/parties Care Plan Implementation Implement interventions Follow-up Actions Evaluate patient outcome Evaluation Review outcome Document outcomes Review interventions Review recommendation/decision Revise/modify interventions OR Close problem/issues/reason/care plan Care orchestration Goals/Outcomes: - Optimize function - prevent/treat symptoms - improve functional capability - improve quality of life - Prevent deterioration - prevent exacerbation and/or - prevent complications - Manage acute exacerbations - Support self management/care Care orchestration Care Plan Stephen Chu 12 April 2011
Issue: What overarching term to use? • Condition • Health concern and care Plans
Issues • What overarching term to use? • Condition: favoured by Care Provision: more neutral than ‘concern’ • Concern: allows for broader set of contexts for care planning, including health maintenance activities • Problem: focus on ‘wrong’ things; not well applicable to pregnancy: NO • Health status: ‘current’ is not a term used • Health issue: many people use it. Europe uses it (e.g. Sweden) • See terms proposed (Susan) • Synonyms: issue, concern • We need to choose, define it and map it to existing terms • Wait for our storyboards and map the correct word to each • Build on existing term work done by reliable sources: HL7 Care Provision, ISO/CEN concepts (Continuity of Care) • Existing glossaries: HL7, CCMC (case management assoc), NLM • Retain meaning of natural language where possible • Use reliable sources • Ian: he has done a term analysis • Note: None of these terms are in the HL7 Core Glossary. See • http://www.hl7.org/v3ballot/html/welcome/environment/index.html
‘Condition’ vs ‘Problem’: From Care Provision (Jan 2011) • …the term “Condition” is used generally in HL7 because it is less negative than “problem,” i.e. management of normal pregnancy or wellness is not considered management of a “problem.” In addition, assessing and optimizing the condition of a patient is considered central to effective healthcare by clinicians. Much of the following is shared by the generalized discussions under Condition List and Condition Tracking. Additional guidance on the use of the Condition List and Condition Tracking structures in the specific use cases of allergy and intolerance is given following the general discussions below. Source: ExplanationandGuidance.pdf document in the Care provision package v3_careprovision_2011JAN.zip
From Kevin Health concern and care plan: new paradigm to define the EHRS • Historically, the EHR was similar to the GHR (Guttenberg Health Record) that was systematically adhered to as it had since Sir. William Osler told us how to treat patients. Often it is even pre-Guttenberg technology dependant (hand written). • This paradigm was implemented in EHRS: PMH, CC, Social Hx, HPI, etc. etc. • This paradigm was somewhat impacted in the 1960’s by crazy Dr. Larry Weed • Every 50 years we need to re-think how we think of patients. • We use information and generate information and actions. • Information used is typically current problems/medications, HPI, and ROS/PE. • Actions are surgery, medical therapy, psychotherapy • We translate what we know into what we do. This defines us and our profession. • So lets formalize it in a model which is optimized to support this
From Kevin What We Know (information) and what we do (actions) • A Health Concern can be linked to any relevant data: labs, encounters, medications, care plan • A Health Concern POV looks like a long hall way, with doors to rooms with all kinds of crap in them. You can, if you read the door name (aka Observaiton.code) query for all of the relevant data (and graph it is numeric, etc.). • At any given instant, what we know is effectively what is in the health concern, and the H&P/initial nursing assessment. • At a given point we have enough information to take action. This action is captured in the Care Plan. Diagnosis or identified problems/concerns then get updated. • For every plan of care there better be some health concern!
From Kevin Health Concern Records what Happens fCare Plan: set of ongoing and future actions GOAL Care Plan and health concern • Care plans need goals, i.e. tries to cause some ObservationEvent to match it. • Care plan has intimate relationship with HealthConcern—is is the reason for the care plan • Can view things via the HealthConcern POV, CarePlan POV, the individual encounter POV, and Health Summary (extraction/view)
Action Items as of 2011-04-13 NB: Completed action items have been removed.
Review of draft list/description of deliverables 2011-04-06 • See wiki: HL7_PCWG_CarePlanDeliverables-Draft-20110405a.doc • Business Requirements, Scope and Vision • Standards context • Storyboards and Use Cases • Interaction diagram • Process Flow • Domain Glossary • Information Model • Business triggers and Rules • Diagram of health concerns/problems and care plan on a timeline? • State machine diagram applied to concerns?? Lifecycle? Status of acts, referrals • Continuity of care timeline • Harmonization (should be in parallel to produce the above to minimize rework)
Care Plan Development - Principles High level processes can be used to guide storyboards, use cases and care plan structure development and activity diagram and interaction diagram Care plan should preferably be problem/issue oriented, although may need to be reason-based where problem/issue not applicable, e.g. health promotion or health maintenance as reason. Use ‘health concern’ as encompassing term? (see Care Provision, 2006-7) Care plan should be goal/outcome oriented- to allow measurement Interventions are goal/outcome oriented External care plan(s) can be linked to specific intervention/care services Goal/outcome criteria are essentially for assessment of adequacy/effectiveness of planned intervention or service Reason for care plan is for guiding care and for communication among care participants. Need to support exchange of information. 2011-04-06 Stephen Chu 5 April 2011
Definition of Care Plan on Wiki • The Care Plan Topic is one of the roll outs of the Care Provision Domain Message Information Model (D-MIM). The Care Plan is a specification of the Care Statement with a focus on defined Acts in a guideline, and their transformation towards an individualized plan of care in which the selected Acts are added. • The purpose of the care plan as defined upon acceptance of the DSTU materials in 2007 is: • To define the management action plans for the various conditions (for example problems, diagnosis, health concerns)identified for the target of care • To organize a plan for care and check for completion by all individual professions and/or (responsible parties (including the patient, caregiver or family) for decision making, communication, and continuity and coordination) • To communicate explicitly by documenting and planning actions and goals • To permit the monitoring, and flagging, evaluating and feedback of the status of goals, actions, and outcomes such as completed, or unperformed activities and unmet goals and/or unmet outcomes for later follow up • Managing the risk related to effectuating the care plan, • Source: http://wiki.hl7.org/index.php?title=Care_Plan_Topic_project