Download
1 / 33
330 likes | 554 Views
Urban Leprosy Elimination. Dr. CR Revankar. MD, DPH Public Health & Leprosy specialist. Contact address : 3-15-14, Garden View Society, Bhavani Nagar, Marol, Andheri-East, Mumbai-400059, India Email: drrevankar50@vsnl.com, macnir@bom3.vsnl.net.in. How important -Urban Leprosy.

E N D
Urban Leprosy Elimination Dr. CR Revankar. MD, DPH Public Health & Leprosy specialist
Contact address: 3-15-14, Garden View Society, Bhavani Nagar, Marol, Andheri-East, Mumbai-400059, India Email: drrevankar50@vsnl.com, macnir@bom3.vsnl.net.in
How important -Urban Leprosy 1.20-25% of the global population is in urban areas & 20-25% of global leprosy case load is likely to be in urban areas (guestimate) 2.Increased transport facilities, scope for employment, attraction for tourism -resulted in increased population movement across the globe Continued
Issue of Global Leprosy Population movement responsible for Infectious disease transmission across the globe-eg. SARS, TB, Leprosy and any other infectious disease. Leprosy should not be considered as a problem of developing countries. Should be considered as a global issue
Objectives After this lecture, one should be able to: Understand the epidemiological trend of leprosy, influencing factors, public health principles and possible strategies to eliminate leprosy in relation to urban population.
Influencing Factors 1.Rapid Industrialization 2.Population migration- Permanent/temporary 3.Migration -intra and inter -slums/residential areas Continued
Influencing factors 4.Increase in population 5.Slum/shanty town growth 6.Congestion, poor hygiene 7.Daily commuters for work from neighboring areas Continued
Influencing factors 8.Socio-economic-cultural aspects 9.Health seeking behavior 10.Complex-health service delivery -Public & Private,modern/traditional, Non-profit health organizations Continued
Influencing factors 11.Catastrophes-Violence, fire, earthquake, demolition of slums for urban planning 12.Fall in economic growth-shifting of labour force to other cities/towns
Special features in slums/shanty towns Fig.1. Demolition Fig.2.Violence Fig.1,2,3 from Bombay Leprosy Project,Bombay Fig.3. Accidental fire
Outcome 1.These environmental and population factors influence the efforts of leprosy elimination in urban areas 2.Continuous growth of urban localities, maintain low level of disease transmission Continued
Outcome 3.Survival of causative organisms, poor living conditions & poor nutrition 4.Difficulty in finding new cases especially-infectious type, relapse 5.Low adherence rate and drop-out from treatment, treatment failure etc.
Recommendations 1.International Leprosy Association-pre-congress workshops: 1973, 1978, 1984, 1988, 1993 2.German Leprosy Relief Association-Urban Leprosy Panel, India: 1975 3.WHO: 1988, 2001 4.Sasakawa Memorial Health Foundation -Singapore International Leprosy Workshop: 1983Continued
Recommendations • 5.Damien Foundation, India: 1998 • 6.Danida Assisted National Leprosy Eradication Program(DANLEP) and National Leprosy Eradication Program, India: 2000 • 7.The Leprosy MissionInternational(TLMI), NewDelhi: 2000 • 8.Indian Association of Leprologists(IAL): 2001
Urban Population Growth Increasing Urban agglomerations with >5 million inhabitants (1950- 2015) in the World. (UN population data, 1999) ___________________________________ Year No. Population (million) ___________________________________ 1950 8 54 1975 22 194 2000 41 417 2015 59 622 ___________________________________
Urban Population Growth 23 megacities by 2015 with more than 10 million population Urban agglomerations (>5 million) endemic for leprosy Bombay, Delhi, Kolkatta, Hyderabad, Chennai, Banglore, Pune, Ahmedabad, Dhaka, Sao Paulo, Rio de Janeiro, Jakarta
Urban slum growth 1.It is estimated that more than 50% of the 12 million population (2001) in Bombay(Mumbai) live in the slums/shanty towns. 60% of them are migrants from other states of India. 2.Poor socio-economic conditions lead to slum/shanty town growth in all towns/cities/metropolitan areas
Impact of MDT Dhaka city -Bangladesh PR/10 000(2002) : 3.45 NCDR/100 000(2001) : 44.86 Smear +ve : 131/2532(5%) (new cases) Migrants : 25% (Jalal Uddin, 2002)
Impact of MDT Delhi-India,2001 PR/10 000(2001) : 4.3 NCDR/ 100 000(2001) : 38.0 Migrants (%) : 40.0 Smear +ve (%) : 9.0 (new cases) Bhagotia, 2002
Impact of MDT Bombay-India,2001 PR/10 000 : 2.3 NCDR/100 000 (2000): 33.0 Migrants : 50%-60% Smear +ve : 560/5131(11%) (new cases) ADHS,Bombay, 2001
Impact of MDT Rio de Janeiro-Brazil,2001 PR/10 000 (2001) : 1.84 NCDR/100 000 (2001) :16.30 Migrants : NA Smear +ve : 252/962 (26.2%) (new cases) Tardin, 2002
Impact of MDT Sao Paulo, Brazil, 2001 PR/10 000 : 0.85 NCDR/100 000 : 2.6 Migrants :Not available Lafratta, 2002
Trend in Leprosy rate in Bombay 12000 10000 8000 No.of cases 6000 4000 2000 0 1992 1993 1994 1995 1996 1997 1998 1999 2000 Prevalenc Detection Infectious ADHS,Bombay,2002
Significant observations 1.New Case detection rate in these megacities/cities has not shown significant reduction for the past 5 years even though prevalence rate showed significant reduction.This is similar to rural leprosy program. continued
Status of infectious leprosy Skin smear positive cases (of public health importance ) from Bombay does not show any significant reduction over the past 5 years. 400-500 (out of 4000-5000 annual new case detection) new infectious leprosy cases are recorded inspite of low prevalence.40-60% are migrants from other parts of India. (ADHS, Bombay, 2001).
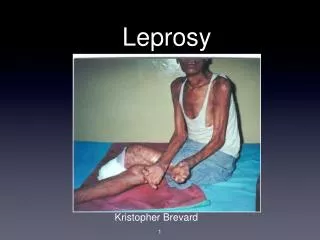
Untreated Lepromatous leprosy cases 2 1 Fig.1,2 from Yawalkar,2002 These cases discharge 240million leprosy germs in 24 hours through nose if untreated (Davey & Rees,1974)
Leprosy Trend in Dharavi slum, Bombay 500 400 300 200 100 0 1981 1979 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 New case Infectious Ganapati R,2002
Migration & Leprosy More than 60% of the skin smear +ve patients(infectious) are migrants to Bombay - maintaining low level of transmission. North America - more than 80% of new leprosy patients are immigrants from other countries maintaining low level of transmission (NHDP Report, 2002).
Leprosy-Migrant population Examination of 72 436 migrant population to different cities/ towns in Maharashtra state,India revealed a detection rate of 194 per 100 000, even though overall Prevalence Rate is coming down in 32 cities/towns (NLEP-Maharashtra,India 1998).
Leprosy- Disability Prevention of Disabilities is not finding its place in the program that it deserves. WHO-AIFO (2000) estimated 3 million leprosy patients with disabilities (including impairments) in the world. Disability case load in urban areas is still not available.
Integration of Leprosy Urban Health services : Public - Private mix programme 1.Government, Municipal medical colleges, hospitals, dispensaries 2.Railway, Industrial hospitals 3.Private hospitals, private doctors 4.Non-profit community organizations