Download
1 / 18
220 likes | 642 Views
RESPIRATORY DISTRESS SYNDROME. By Dr. Gacheri Mutua. DEFINITION. Also known as Hyaline Membrane Disease Is a respiratory disorder that affects newborns More common in premature infants especially born 6wks or more before their due date

E N D
RESPIRATORY DISTRESS SYNDROME By Dr. Gacheri Mutua
DEFINITION • Also known as Hyaline Membrane Disease • Is a respiratory disorder that affects newborns • More common in premature infants especially born 6wks or more before their due date • Their lungs have insufficient surfactant, necessary to maintain lung compliance
Disease is exacerbated by: • Cold stress • Hypoxia • Acidosis • Sepsis • Natural history- clinical signs develop within 6hrs of life with progressive worsening over the first 48 to 72hrs of life
Predisposing factors • Prematurity • Male gender and are more likely to die from the disease • Caucasian > black • Caesarean section • Low APGAR score • Maternal diabetes • Congenital hypothyroidisim • Familial predisposition • Twins • Postnatal hypothermia • Maternal malnutrition • Intrauterine growth retardation • Hemolytic disease of the newborn
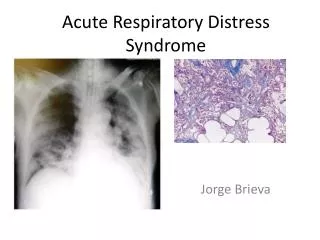
DIAGNOSIS • Clinical:- • tachypnoea • grunting respirations • intercostals recession, sternal indrawing • nasal flaring • cyanosis • increased oxygen requirements • deranged cardiovascular parameters: HR, BP • Radiological features:- • Air bonchograms with characteristic ground glass appearance • Haematological:- • anaemia • Thrombocytopenia • Blood gas measurements • Mixed metabolic and respiratory acidemia
PREVENTION • Prevent premature delivery • Antenatal steroid therapy • Drugs to mature surfactant synthetic pathways: aminophylline • Prevent asphyxia • Avoid drugs that cause respiratory depression • The course of the disease is altered by exogenous surfactant therapy and assisted ventilation
MANAGEMENT • Non-respiratory • Temperature control • Avoid enteral feeding • IV therapy 5% or 10% dextrose • Closely monitor blood glucose • Antibiotics: penicillin, gentamicin • Assess the baby's circulatory status by monitoring heart rate, peripheral perfusion, and blood pressureAdministerblood or volume expanders, and use appropriate vasopressors to support circulation where necessary.
Respiratory • Airway- place infant in lateral or prone posture rather than supine • Repeated suctioning of pharynx is not required and may cause apnoea and hypoxia
Oxygen • Administer humidified oxygen at flow rates of 6-8l/min • Monitor arterial blood gases, aim to keep pO2 between 50 and 80mmHg • Desired range of monitored pulse oxymeter for infants <34weeks gestation is 88 to 95% but for more mature infants 88 to 100%
INTUBATION AND IPPV • IPPV- Intermittent Positive Pressure Ventilation • Indications: • Cyanosis that persists in spite of maximal oxygen therapy • Severe recurrent apnoea • Respiratory failure (pCO2 >70 and pH <7.2)
CPAP • Continuous Positive Airway Pressure is used to treat preterm infants whose lungs have not yet fully developed such as in RDS or bronchopulmonarydysplasia • It’s functionally similar to PEEP, except that PEEP is an applied pressure against exhalation and CPAP is a pressure applied by a constant flow • CPAP:- • improves survival • decreases the need for steroid treatment for their lungs • decreases the need for IPPV
Surfactant ventilator settings • Ventilator rate 60 breaths per minute • Inspiratory time 0.3sec; expiratory time 0.7sec • PEEP 5cm • Oxygen set to maintain saturations of 88 to 95% • Peak inspiratory pressure (PIP) 20-30cm water
SURFACTANT ADMINISTRATION • Premature neonates with surfactant deficiency and respiratory distress syndrome have an alveolar pool of about 5mg/kg. Full-term animal models have pools of 50-100mg/kg. • Recommended dosages of clinically available surfactant preparations are 50-200mg/kg, approximately the surfactant pool of term newborn lungs
Rapid bolus administration of surfactant after adequate lung recruitment with 3-4cm of positive end-expiratory pressure (PEEP) and adequate positive pressure may improve its homogeneous distribution. • Most neonates require 2 doses; however, as many as 4 doses, given at 6-hour to 12-hour intervals, were used in several clinical trials. • NB: • Dosages could be given as a rapid bolus or intermittent administration. • Prophylactic doses can be given soon after delivery
If the patient rapidly improves after 1 dose, respiratory distress syndrome is unlikely. • Conversely, in infants who have a poor or no response, patent ductus arteriosus (PDA), pneumonia, and complications of ventilation (air leak) should be excluded, especially before subsequent surfactant doses are given.
SUDDEN DETERIORATION • In spontaneously ventilating: • pneumothorax • failure of oxygen supply • increase in severity of the underlying disease • In a ventilated infant: • pneumothorax • endotracheal tube blockage or displacement • mechanical failure with the ventilator • increase in the severity of the underlying lung disease • massive intraventricular haemorrhage • necrotizing enterocolitis, especially if perforation has occurred • patent ductus arteriosus
FAMILY PSYCHOTHERAPY • Staff members (preferably a physician and a nurse) should keep the patient’s parents well informed by frequently talking to them, especially during the acute stage of respiratory distress syndrome