Download
1 / 41
500 likes | 1.21k Views
ACUTE RESPIRATORY DISTRESS SYNDROME. Dr. Poonam Patel. University College of Medical Sciences & GTB Hospital, Delhi. ARDS. Definition Diagnosis Risk factors Pathophysiology Clinical features Management. ARDS.

E N D
ACUTE RESPIRATORY DISTRESS SYNDROME Dr. Poonam Patel University College of Medical Sciences & GTB Hospital, Delhi
ARDS • Definition • Diagnosis • Risk factors • Pathophysiology • Clinical features • Management
ARDS • Severe, acute lung injury involving diffuse alveolar damage, increased microvascular permeability and non cardiogenic pulmonary edema • First defined by Ashbaugh and colleagues in 1967. • Milder form of ARDS is Acute lung injury (ALI).
American European Consensus Conference Criteria for ALI & ARDS
CARDIOGENIC VS NON-CARDIOGENIC EDEMA Cardiogenic Non-cardiogenic 1. Prior h/o cardiac disease Absence of heart disease 2. Third heart sound No third heart sound 3. Cardiomegaly Normal sized heart 4. Infiltrates:Central distribution Peripheral distribution 5. Widening of vascular pedicle ( width of mediastinum) Normal width of vascular pedicle 6. PA wedge pressure N or PA wedge pressure 7. Positive fluid balance Negative fluid balance
ARDS exudative and fibrotic phases Exudative (acute) phase Fibrotic phase
Murray & Mathay Lung Injury Score Chest X film findings • Alveolar consolidation Score One quadrant 1 Two quadrant 2 Three quadrant 3 Four quadrant 4 Oxygenation status (Hypoxemia Score) • PaO2 / FiO2 Score > 300 mmHg 0 225-299 mmHg 1 175-224 mmHg 2 100-174 mmHg 3 < 100 mmHg 4
Pulmonary compliance • Compliance (ml/cmH2O) Score • > 80 0 • 60-79 1 • 40-59 2 • 20-39 3 • < 19 4 • PEEP settings • PEEP (cmH2O) Score • < 5 0 • 6-8 1 • 9-11 2 • 12-14 3 • > 15 4
Acute lung injuries are assessed by dividing sum of above points by 4, if: • 0 points No pulmonary injury • 1-2.5 points Mild to moderate • > 2.5 points Severe (ARDS)
RISK FACTORS Direct Lung Injury • Pneumonia • Aspiration of gastric contents • Toxic inhalation • Near drowning • Pulmonary contusion • Fat embolism • Reperfusion pulmonary oedema - post lung transplantation or pulmonary embolectomy (N.Engl J Med 2000)
RISK FACTORS Indirect lung injury • Sepsis • Severe trauma • Acute pancreatitis • Cardiopulmonary bypass • Massive transfusions • Drug over dose
ARDS MECHANISM OF LUNG INJURY • Activation of inflammatory mediators and cellular components resulting in damage to capillary endothelial and alveolar epithelial cells • Increased permeability of alveolar capillary membrane • Influx of protein rich edema fluid and inflammatory cells into air spaces • Dysfunction of surfactant
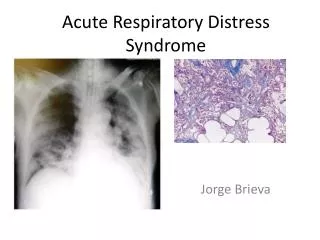
HISTOPATHOLOGY Exudative phase (1st week) • Alveolar and interstitial edema • Capillary congestion • Destruction of Type I alveolar cells • Early hyaline membrane formation Proliferative Phase (2nd to 4th week) • Increased type II alveolar cells • Cellular infiltration of alveolar septum • Organisation of hyaline membranes Fibrosis Phase (>3 to 4 weeks) • Fibrosis of hyaline membranes and alveolar septum • Alveolar duct fibrosis
INFLAMMATORY MEDIATORS IN ARDS IL-1, IL-6, IL-8 MIP -1α Endothelin 1 VWF Endotoxin Fas ligand
PATHOPHYSIOLOGY • Refractory hypoxemia – shunting, dead space ventilation • Alveolar collapse – surfactant dysfunction, fluid filled alveoli. • Decreased lung compliance
CLINICAL FINDINGS IN ARDS Phase 1 Acute Injury • Normal physical examination and chest X- Ray • Tachycardia, Tachypnea, Respiratory alkalosis Phase 2 Latent Period • Lasts approximately 6-48 hrs. after injury • Patient appears clinically stable • Hyperventilation and hypocapnia persists • Mild increase in work of breathing • Widening of alveolar-arterial oxygen gradient • Minor abnormalities on physical examination and chest x-ray
Phase 3 Acute Respiratory Failure • Marked tachypnea and dyspnea • Crepts • Decreased Lung Compliance • Diffuse infiltrates on chest x-ray • Phase 4 Severe Abnormalities • Severe Hypoxemia unresponsive to therapy • Metabolic and respiratory acidosis
MANAGEMENT OF ARDS • Control of the causative factor • Analgesia, antibiotics, sedation • Nutritional support • Optimization of hemodynamics • Mechanical ventilation • Adjuncts to low tidal volume ventilation • Restrictive (dry) fluid management • Permissive hypercapnia • Prone positioning • Recruitment maneuvers
MANAGEMENT OF ARDS • Salvage intervention for patients with severe hypoxemia with ARDS • Tracheal gas insufflation • Inverse ratio ventilation • ECMO • HFOV • Inhaled (NO, prostacyclin) • corticosteroid
VENTILATORY STRATEGY IN ARDS PATIENTS • Traditional approach • Open lung approach • Lung protective ventilatory approach • NIH NHLBI ARDS Clinical Network
OPEN LUNG APPROACH On Static Pressure Volume curve of lung • Lower Inflection Point (Pflex) – most recruitable alveoli opened, below which alveolar closure is hypothesized to occur • Upper Inflection Point (UIP) – beyond which overdistention of alveolar units occurs, • PEEP set 2 cm H2O above Pflex
OPEN LUNG APPROACH • Maintaining inflation & deflation between 2 inflection points during entire respiratory cycle is called Open Lung Ventilation • Ventilatory setting where PEEP >Pflex & T.V is reduced so that Pplat < UIP is basis for lung protective strategies • Advantages - avoids repetitive opening & closing of alveoli (AELECTRAUMA) • Traditional PEEP vs High PEEP study – ALVEOLI Trial
ARDSnet protocol • Calculated predicted body weight (PBW) • Male: 50+2.3[height(inches)-60] • Female: 45.5+2.3[height(inches)-60] • Mode: Volume assist-control • Change rate to adjust minute ventilation (not>35/min) • pH goal 7.30-7.45 • Plateau press<30cm H20 • PaO2 goal: 55-80mmhg or SpO2 88-95% • FiO2/PEEP combination to achieve oxygenation goal
ARDSnet protocol • PEEP/FiO2 relationship to maintain adequate PaO2/SpO2 • PaO2 goal: 55-80mmHg or SpO2 88-95% use FiO2/PEEP combination to achieve oxygenation goal FIO2 PEEP
PERMISSIVE HYPERCAPNIA • Strategy to minimize VILI • Low tidal volume & low peak airway pressures • CO2 retention occurs • Role of alkali ? • Contraindications – raised ICP acute CVA myocardial ischemia pulmonary hypertension uncorrected severe metabolic acidosis sickle cell anemia pregnancy ,
INVERSE RATIO VENTILATION • I:E ratio > 1 • Improvement in oxygenation by – increases mean airway pressure, auto PEEP, decreased deadspace ventilation, improved V/Q mismatch, reduced intrapulmonary shunting. • Advantages- lower peak alv press, ↑ FRC, ↓ed dead space ventilation, easily given through modern ventilators. • Disadvantages– barotrauma, sedation/muscle paralysis required, worsening pulmonary edema.
PRONE POSITION VENTILATION • The prone ventilation of patients with ARDS first described in the 1970s • Large RCT by Gattinoni and colleagues • Suggested mechanisms include • Better ventilation – perfusion matching from alteration in regional blood flow • Increase in functional residual capacity • Alteration in respiratory mechanics and the creation of more uniform lung expansion. Change in regional diaphragm motion • Recruitment of collapsed alveoli • Better clearance of secretions
PROBLEMS OF PRONE POSITION • Facial edema • Airway obstruction • Difficulties with enteral feeding • Vascular and nerve compression • Loss of venous accesses and probes • Loss of chest drain and catheters • Accidental extubation • Apical atelectasis • Increased need for sedation • Pressure sores
CONTRAINDICATIONS OF PRONE POSITION VENTILATION • Unstable spine • Head injury with raised ICP • Unstable Cardiac rhythm • Severe abdominal and soft tissue infection
LIQUID VENTILATION • Perflurocarbons carry 50ml/100ml of O2 & 200ml/100ml of CO2 • FRC filled with warmed, oxygenated PFC & pt ventilated from conventional ventilator • Mechanism – alveolar recruitment, promotes oxygenation, anti inflammatory action, attenuates VILI. • Disadvantage – high density
FLUID MANAGEMENT • Controversy regarding type of fluid • Acute Respiratory Distress Network Study 05 (ARDSNet 05) Fluid and Catheter Treatment Trial (FACTT) - conservative strategy of fluid management is associated with improved lung function and shortened duration of mechanical ventilation and intensive care without increasing non pulmonary-organ failures. (NEJM June 15, 2006; Vol 354, No. 24, pp 2564-75; NEJM May 25, 2006; Vol 354, No. 21, pp 2213-24)
NITRIC OXIDE IN ARDS • NO is a selective pulmonary vasodilator • NO acts selectively on well ventilated alveoli bypassing fluid filled or collapsed alveoli • Improve ventilation-perfusion mismatch • NO – immunomodulator • Very costly • C/I – absolute methemoglobinemia, relative bleeding diathesis, intracranial bleed, severe LVF
ROLE OF OTHER DRUGS • Surfactant therapy • Surfactant dysfunction exist in ARDS, surfactant decreases alveolar surface tension and alveolar edema • Anticytokine effect – inhibition of IL-1, IL-6, TNF • Steroids • Routine use – not advocated esp. in acute phase • NSAIDs • Inhibit prstaglandin pathways esp. indomethacin and ibuprofen • Other agents • Ketoconazole – inhibit Tx synthesis • Pentoxyphylline
COMPLICATIONS ASSOCIATED WITH ARDS • Pulmonary: barotrauma (volutrauma), pulmonary embolism, pulmonary fibrosis, ventilator-associated pneumonia (VAP), Oxygen Toxicity • Gastrointestinal: haemorrhage (ulcer), dysmotility, pneumoperitoneum, bacterial translocation • Cardiac: Arrhythmias, myocardial dysfunction • Renal: acute renal failure (ARF), Fluid retention • Mechanical: vascular injury, tracheal injury/stenosis (result of intubation and/or irritation by endotracheal tube) • Nutritional: malnutrition, anaemia, electrolyte deficiency • Hematologic: DIC, thrombocytopenia, anemia • Infection: sepsis, nosocomial pneumonia
REFERENCES • Christie JD, Lanken PN. Acute lung injury and the acute respiratory distress syndrome. Critical Care – Hall • Harrison’s Principle of Internal Medicine, 16th ed. • Foner BJ, Norwood SH, Taylor RW. Acute respiratory distress syndrome. Critical Care, 3rd ed. Civetta • Allen B. Gilman, Parsons E. Polly.acute respiratory failure due to ARDS and pulmonary edema. Critical care-Irwin & Rippe, 6th edition. • Mechanical ventilation – Chang, 2nd ed. • NIH NHLBI ARDS Clinical Network - Mechanical Ventilation Protocol Summary 2000 • Wiener-Kronish JP, et al. The adult respiratory distress syndrome : definition and prognosis, pathogenesis and treatment. BJA 1990; 65: 107-129.