Download
1 / 28
330 likes | 1.43k Views
Acute Respiratory Distress Syndrome. Outline. Definition Low tidal volume ventilation (6 mL/kg of predicted body weight) Plateau pressure Permissive hypercapnia Hypoxemia (PEEP/FiO2) Prone ventilation Neuromuscular blockade Conservative fluid management. ARDS.

E N D
Outline • Definition • Low tidal volume ventilation (6 mL/kg of predicted body weight) • Plateau pressure • Permissive hypercapnia • Hypoxemia (PEEP/FiO2) • Prone ventilation • Neuromuscular blockade • Conservative fluid management
ARDS At it’s core, ARDS is non-cardiogenic pulmonary edema.
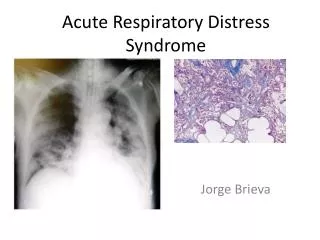
ARDS • Definition: • ARDS is, in essence, non-cardiogenic pulmonary edema • Clinically characterized by bilateral pulmonary infiltrates on imaging with hypoxemia that is not due to congestive heart failure • Hypoxemia in terms of PaO2/FiO2 ratio defines severity of ARDS
ARDS Etiologies • Sepsis • Because sepsis is the most common cause of ARDS, the management of ARDS is part of the Surviving Sepsis Guidelines • Aspiration • Pneumonia • Severe trauma • Massive transfusions • Pancreatitis
ARDS Highlights • Best evidence with mortality benefit • Low tidal volume ventilation (6 mL/predicted body weight in kg) • Need to have a height on every patient to calculate predicted body weight • In severe ARDS (PaO2/FiO2 < 150) • Prone ventilation • Neuromuscular blockade with cis-atracuriumfor 48 hours • Other things that can be tried • Inhaled nitric oxide (no mortality benefit) • Recruitment maneuvers (no mortality benefit)
ARDS Highlights • Once septic shock is over, keeping the patient dry is beneficial • Can help liberate from mechanical ventilation faster without increased renal failure
Acute Respiratory Distress Syndrome • Low tidal volume ventilation has been shown to be provide mortality benefit • Need to measure height for every patient in the ICU • Low tidal volume ventilation is based on predicted body weight • Dependent on height of patient • Neuromuscular blockade with cis-atracurium for 48 hours is beneficial in severe ARDS (PaO2/FiO2 < 150 mmHg) • Prone ventilation is beneficial in severe ARDS (PaO2/FiO2 < 150 mmHg)
Low Tidal Volume Ventilation • NEJM 2000 trial suggested decreased mortality in patients ventilated at a tidal volume of 6 mL/kg of predicted body weight compared to 12 mL/kg of predicted body weight • Based on ideal body weight (kg) • Male: 50 + 0.91(centimeters of height – 152.4) • Female: 45.5 + 0.91(centimeters of height – 152.4) • All the patients were ventilated on volume assist-control mechanical ventilation
Low Tidal Volume Ventilation • Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome NEJM May 4, 2000
ARDS Net Protocol • Given the decrease in mortality with low tidal volume ventilation, the ARDS Net protocol is the standard of care for patients with ARDS • The initial tidal volume is set at 8 mL/kg of predicted body weight and titrated down to 6 mL/kg of predicted body weight • It is important to know the height of the patient or have it measured, as the predicted body weight (ideal body weight) is calculated from the height of the patient • The ARDS Net protocol is given on the next two slides
Plateau Pressure • Mentally separate the lungs into the airways and the lung parenchyma • The plateau pressure is the pressure required to inflate the lung parenchyma (without the pressure required to push the air through the airways) Airways Lung Parenchyma
Plateau Pressure • In volume ventilation, when the ventilator pushes air into the patient, the pressure required is a sum of the pressure needed to overcome the resistance of the airways and the pressure required to inflate the lung parenchyma • Total pressure = Pressure to overcome resistance of airways + Plateau pressure (Pressure to inflate lung parenchyma) Airways Lung Parenchyma
Plateau Pressure Goal • Plateau pressure is obtained by performing an end-inspiratory pause when the patient is vented in a volume mode of ventilation • This is a measure of the pressure seen by the lung parenchyma after it is inflated by the ventilator • Plateau pressure can be thought of as a surrogate for how “stiff” the lungs • For a given tidal volume of ventilation, the higher the plateau pressure, the “stiffer” the lungs are • If you think of the lung parenchyma as a balloon, a stiffer balloon (lung) will take more pressure to inflate while inflating a less stiff balloon (lung) to the same volume will take less pressure
Plateau Pressure Goal • In ARDS, the goal plateau pressure is < 30 cm H2O as this was part of the ARDS Net trial protocol • If the plateau pressure is > 30 cm H2O, the ARDS Net protocol recommends decreased the tidal volume by 1 mL/kg of predicted body weight • To a minimum of 4 mL/kg of predicted body weight • To understand why lowering the tidal volume lowers the plateau pressure, again think of the lung parenchyma as a balloon. • If inflating the balloon to 500 mL requires a pressure of 35 cm H2O (this would be the plateau pressure), then inflating the same balloon to 400 mL will lower the pressure required as you are not inflating the balloon as much
Permissive Hypercapnia • Permissive hypercapnia • Because of the mortality benefit with low tidal volume ventilation, the pCO2 of the patient is allowed to rise. • For patients in ARDS, the pH is allowed to drift down to 7.30 • If the pCO2 rises with low tidal volume ventilation but the pH is > 7.30, there is no need to change the tidal volume as the body tolerates acidemia fairly well
Hypoxemia • The hypoxemia associated with ARDS is secondary to alveoli that are “flooded” because of increased pulmonary vascular permeability
Hypoxemia • The hypoxemia associated with ARDS can be corrected by increasing PEEP and/or FiO2 • The increased PEEP (peak end expiratory pressure) allows recruitment of alveoli that are “flooded” secondary to the increased pulmonary vascular permeability due to ARDS • This recruitment of alveoli helps to improve oxygenation • Increasing FiO2 (inspired oxygen concentration) can also improve oxygenation by increasing the oxygen gradient from the inspired air to the patient’s blood
PEEP in ARDS • There is no mortality benefit between low PEEP versus high PEEP • NEJM 2004 • Cochrane Review 2013 • Using higher PEEP versus lower PEEP will increase oxygenation
Prone Positioning in Severe Acute Distress Syndrome • Guerin et al Prone Positioning in Severe Acute Distress Syndrome NEJM 2013 • In patients with ARDS where Pa/FiO2 < 150 mmHg, there was decreased mortality in patients that received prone positioning while being mechanically ventilated compared to supine positioning • Results • 28 day mortality: 16% prone vs. 32.8% supine (p < 0.001) • 90 day mortality: 23.6% prone vs. 41% supine (p < 0.001)
Prone Positioning in Severe Acute Distress Syndrome • Because edema becomes gravitationally dependent in supine ARDS patients, prone positioning improves oxygenation by increasing alveoli recruitment of those alveoli that have been “flooded”
Neuromuscular Blockade in ARDS • Papazian et al Neuromuscular Blockers in Early Acute Respiratory Distress Syndrome NEJM September 16, 2010 • Decreased mortality using the neuromuscular blocker (cis-atracurium) in ARDS patients with PaO2/FiO2 < 150 • Cis-atracurium was used only for the first 48 hours after enrollment into the trial • There was no difference in ICU-acquired paresis between groups (placebo versus cis-atracurium) • This is important because previous studies have suggested that the use of neuromuscular blockers (paralytics) have been associated with ICU-acquired paresis
Conservative Fluid Management in ARDS • After the initial septic shock is over, a conservative fluid management in ARDS patients is associated with increased ventilator free days and ICU free days, without increasing mortality or renal failure requiring initiation of hemodialysis • Comparison of Two Fluid-Management Strategies in Acute Lung Injury NEJM June 2006 • In patients without hypoperfusion, the conservative fluid management group had a CVP goal of < 4 mmHg • In comparison, the liberal fluid management group had a CVP goal of 4-8 mmHg • This was accomplished with the use of diuretics in patients that were not on vasopressors and did not show signs of hypoperfusion