Download
1 / 33
381 likes | 1.05k Views
Acute respiratory distress syndrome. Prof.M.K.Arora Dr.Lenin Dr.Prabhu. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. History. Described by Ashbaugh et al in 1967 Acute respiratory distress in adults Ashbaugh DG et al .Lancet 1967

E N D
Acute respiratory distress syndrome Prof.M.K.Arora Dr.Lenin Dr.Prabhu www.anaesthesia.co.inanaesthesia.co.in@gmail.com
History • Described by Ashbaugh et al in 1967 Acute respiratory distress in adults Ashbaugh DG et al .Lancet 1967 • “Adult respiratory distress syndrome” Term was coined by Petty TL, Ashbaugh DG. Chest 1971
Other names • Adult hyaline-membrane disease • Adult respiratory insufficiency syndrome • High output respiratory failure • Congestive atelectasis • Hemorrhagic lung syndrome • Da Nang lung • Stiff-lung syndrome • Shock lung • White lung Taylor RW et al Res Medica 1983;1:17-21.
Definition • Lung injury score • Modified lung injury score • NAECC Definition
Definition • Three part expanded definition • Part 1- acute or chronic on course • Part 2- lung injury score • Part 3- associated risk factors such as sepsis, pneumonia, aspiration or major trauma Murray JF, Matthay MA 1988
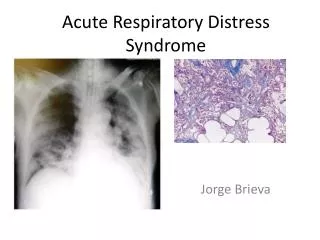
Lung injury score • Chest radiograph • Hypoxemia score • PEEP score • Respiratory compliance score
CXR No consolidation ..0 Confined to 1 quadrant …………1 2 quadrant ……….2 3 quadrant ……….3 4 quadrant ……….4 PaO2/FiO2 >300……..0 225-299 …1 175-224 …2 100-174 …3 <100……..4 Lung injury score…
PEEP (when mechanically ventilated) <5 cm H2O……..0 6-8 cm H2O ……1 9-11 cm H2O …..2 12-14 cm H2O ....3 >15 cm H2O …...4 Compliance (when available) >80 ml/ cm H2O …..0 60-79 ml/ cm H2O ...1 40-59 ml/ cm H2O …2 20-39 ml/ cm H2O …3 <19 ml/ cm H2O …...4 Lung injury score…
Lung injury score… Add the sum of each component and divide by the number of components used 0- No lung injury 0.1-2.5 – Mild to moderate lung injury >2.5 – Severe lung injury (ARDS)
Modified lung injury score • PaO2/FiO2 <174 • Bilateral infiltrates on chest x-ray
NAECC Definition 1994,1998 • Onset- acute and persistent • Oxygenation criteria PaO2/FiO2≤ 300 for ALI PaO2/FiO2≤ 200 for ARDS • Exclusion criteria- PAOP ≥ 18 mmHg Clinical evidence of left atrial hypertension • Radiographic criteria- bilateral opacities consistent with pulmonary edema Bernard GR et al 1994
Common Aspiration pneumonia Pneumonia Less common Inhalational injury Pulmonary contusion Fat emboli Near drowing Reperfusion injury Asso. clinical disorders-direct
Common Sepsis Severe trauma Multiple fractures Multiple blood transfusion Less common Acute pancreatitis Cardiopulmonary bypass DIC Burns Head injury Asso. clinical disorders-indirect
Risk factors predictive of mortality • Liver dysfunction/ cirrhosis • Sepsis • Non pulmonary organ dysfunction • Age > than 65 • Organ transplantation, HIV, active malignancy, chronic alcoholism, mechanim of lung injury
Pathogenesis Lung injury • The pulmonary response to a broad range of injuries occuring either -directly to the lungs -or as the consequence of injury or inflammation at other sites in the body
Acute Exudative Phase Exudative phase • Commencing within 24 hrs • 1-7 days • Diffuse alveolar damage • Diffuse Microvascular injury • Neutrophil infiltration • Edematous alveolar wall • Hyaline membrane
Acute Exudative Phase • Basement membrane disruption • Type I pneumocytes destroyed • Type II pneumocytes preserved • Surfactant deficiency • inhibited by fibrin • decreased type II production • Microatelectasis/alveolar collapse • Self limited or progresses
Proliferative phase • For 3-10 days • Type II pneumocyte • proliferate • differentiate into Type I cells • reline alveolar walls • Fibroblast proliferation • interstitial/alveolar fibrosis
Fibrotic Phase • 1-2 weeks • Characterized by: • local fibrosis • vascular obliteration • Repair process: • resolution vs fibrosis
Pathophysiology • Interstitial / alveolar edema • Severe hypoxemia • due to intra-pulmonary shunt • High ventilatory demands • high metabolic state • increased VD/VT • decreased lung compliance • Pulmonary HTN
Clinical features- CHF & ARDS • Anxiety, dyspnea, tachypnea • Reduced lung volumes • Decreased lung compliance • ABG- respiratory alkalosis, hypoxemia • CXR
Favour of ARDS • ARDS risk factors • PCWP • BALF is proteinaceous and inflammatory • Pathological findings
Diagnosis • Based on clinical criteria • no diagnostic tests • Confirmatory tests: • PA catheter • PAWP = normal/reduced • [bronchial secretion protein]:[serum protein] • ratio > 70% - 80% • CT scan-heterogenous pattern with a predominance of infiltration in the dependent region
Differential Diagnosis • Cardiogenic pulmonary edema • Bronchopneumonia • Hypersensitivity pneumonitis • Pulmonary hemorrhage • Acute interstitial pneumonia (Hamman-Rich Syndrome) www.anaesthesia.co.inanaesthesia.co.in@gmail.com