Download
1 / 20
210 likes | 435 Views
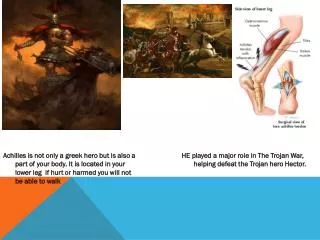
ACHILLES TENDONITIS AND RUPTURE. Dr Carl Clinton (no conflict of interests). Will not include such pathologies:- a) Retrocalcanel Bursitis b) Haglund’s Deformity c) Impingement Syndrome e) ‘Pump Bump’ e) Ankle O/A f) Ruptured Bakers’s Cyst g) DVT. ANATOMY 1.

E N D
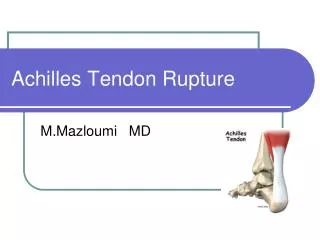
ACHILLES TENDONITISAND RUPTURE Dr Carl Clinton (no conflict of interests)
Will not include such pathologies:- a) Retrocalcanel Bursitis b) Haglund’s Deformity c) Impingement Syndrome e) ‘Pump Bump’ e) Ankle O/A f) Ruptured Bakers’s Cyst g) DVT
ANATOMY 1 a) Attaches the plantaris/ gastrocnemius and soleus muscles to the calcaneus b) Thickest and strongest tendon in the body c) Achilles muscle reflex tests the integrity of the S1 spinal root d) About 15cm (6in) long
ANATOMY2 e) The tendon can receive a load stress 3.9 times body weight during walking and 7.7 times body weight during running f) The tendon is surrounded by a connective tissue sheath (paratenon) rather than a true synovial sheath
ANATOMY 3 g) Arterial anatomy of Achilles - supplied by two arteries - the posterior tibial - the peroneal arteries - 3 vascular territories - the midsection supplied by the peroneal artery - promixal and distal section supplied by the posterior tibial artery The midsection of Achilles markedly more hypovascular (risk rupture and surgical complications at its midsection).
EPIDEMIOLOGYANDCAUSES a) OVERUSE - too long/too fast/too steep/ too explosive b) MISALIGNMENT - gait (excessive pronation) c) IMPROPER FOOTWEAR - saddle too low/extra dorsiflexion e) MEDICAL SIDE EFFECTS - quinolone group of A/B (ciprofloxacin) e) CORTISONE- indirect - weakened Achilles feels too comfortable g) ACCIDENTS - laceration/crush h) GENETICS - individuals with the single nuclear plymorphism (SNP) TT genotype of the GDF5rs 143383 variant have twice the risk of developing Achilles problems i) SYSTEMIC CONDITIONS - gout/RA/SLE/Cushing’s syndrome
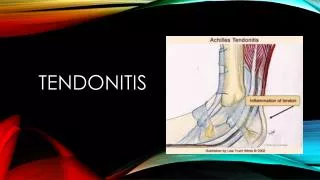
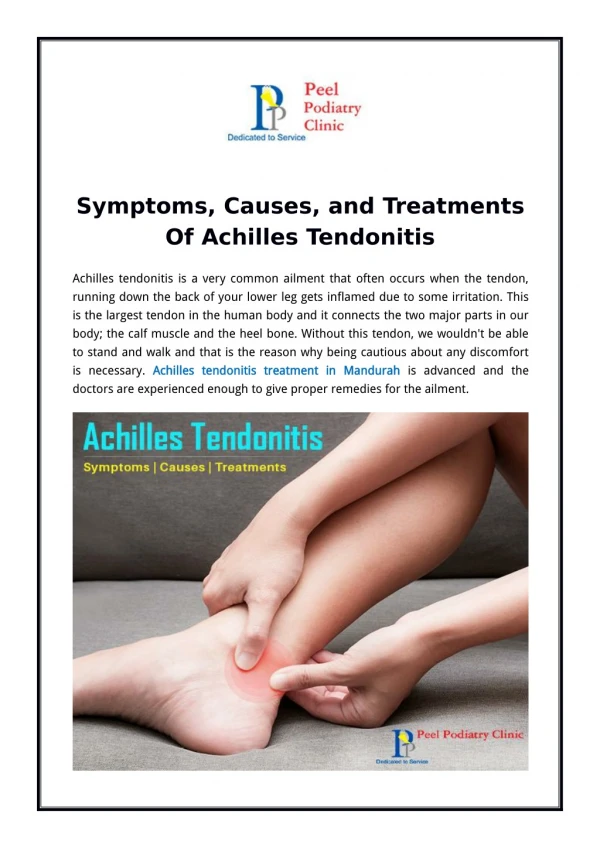
PRESENTATION a) ACHILLES TENDONITIS - gradual onset pain/stiffness - improves with heat and exercise ‘able to run off symptoms’ - may with strenuous activity get worse or experience calf pain - tenderness of the tendon on palpation - there may be crepitus and swelling - may be pain on active movement of the ankle joint
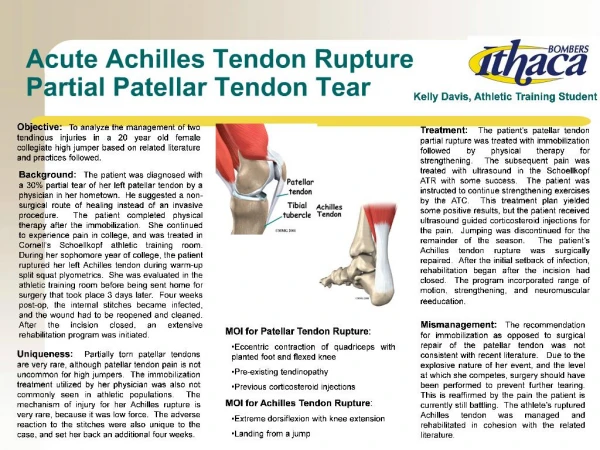
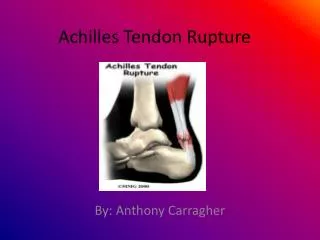
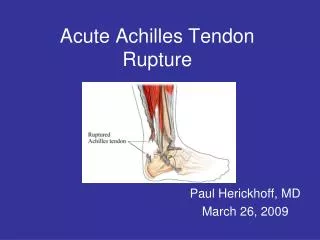
PRESENTATION b) ACHILLES RUPTURE - rupture can occur at any age but most common 30 - 50 year old - acute onset of pain in tendon - sudden ‘sharp pain’ - snap ‘heard’ - may have PMH of Achilles Tendonitis - inability to stand on tiptoe - altered gait ‘inability to push off’ - swelling/ GAP
EXAMINATION - observe gait - look for swelling/bruising - may have a palpable GAP - active plantar flexion is weak or absent - ‘Thompson’s Test’ ‘calf squeeze test’ - fusiform swelling with pain to palpation - gout/RA/SLE/Cushings’ Syndrome/DVT/ ruptured Bakers’s Cyst/O/A ankle (examine ankle/knee/calf)
INVESTIGATIONS - UTRASOUND - MRI
MANAGEMENT ACHILLES TENDONITIS Insufficient evidence from randomised controlled trials to determine which method of treatment is the most appropriate.
a) abstain from aggravating activities b) NICER - ?? Use NSAID (inflammation v degenerate) c) physio + relative rest (alternative exercise) Podiatrist - ‘stretching/strengthening’ Hip/back muscles tight Calf muscles tight Strengthening anterior tibialis - massage - eccentric exercises - orthotics (gait) / review footwear
d) physical therapy - US/electric stimulation/laser photo stimulation e) other treatments - heparin - steriod injections/sclerosant injections - glycosaminoglycan sulfate - actovegin - GTN patches - electronic wave shock treatment - extra corporeal shockwave therapy - blood letting/blood injections - needling - casting
f) surgery -? last resort - ? after six months - ? plantaris wrap around - ? foot in equinus in plaster 6/52 - ? degenerate v inflammatory
MANAGEMENT ACHILLES RUPTURE SURGICAL V CONSERVATIVE a) surgery v non surgery ‘NO CONSENSUS’ :- b) best surgical approach c) best non-surgical approach
Surgical treatment of Acute Achilles Rupture significantly reduces the risk of re-rupture compared with non-surgical treatment, but produces significantly higher risks of other complications such as infection, adhesions and disturbed skin sensibility/breakdown.
PROGNOSIS ACHILLES TENDONITIS a) no consensus on best treatment b) recovery can take weeks or months c) surgery is possible
PROGNOSIS ACHILLESRUPTURE a) no consensus on best treatment b) surgical treatment decreased risk of re- rupture c) may take 1 year to recover d) may be left with slight loss of function e) usually good prognosis however
ANY QUESTIONS ? July 2013