Download
1 / 36
360 likes | 446 Views
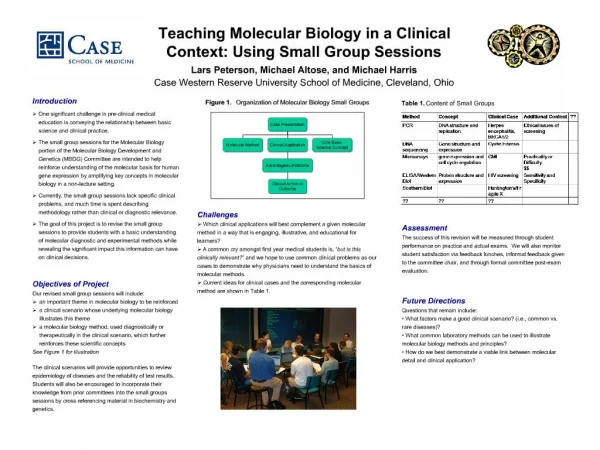
Improving the Care of Diabetic Patients in a Primary Care Practice via Affiliation with a Multi-Site Accountable Care Organization. Team: Mary Dallas, David Madison, Michael Peterson, Natalie Schwartz. Consulting Project.

E N D
Improving the Care of Diabetic Patients in a Primary Care Practice via Affiliation with a Multi-Site Accountable Care Organization Team: Mary Dallas, David Madison, Michael Peterson, Natalie Schwartz
Consulting Project • Client: Best Health Medical Associates, 10 physician primary care group, Epic EMR, joined a local ACO • Location: Multiple clinics, Chicago area • Affiliated Hospital: Columbia West, 700 beds, GE Centricity EMR • Ancillary Services: 3 different reference labs, 3 retail pharmacies • Goal: Diabetes Care Improvement Project to manage diabetic patients in ACO
Deliverables • Assessment of current technology platform and information gaps related to patient care • Recommend technology solutions to address information gaps with ROI estimation • Reports to identify ACO patients and monitor quality and cost of care
ACO – The Shared Savings Model • 3 year agreement for participating providers • 2 options: one sided model, or two sided model • 1st year participation consist primarily of reporting, and quality and utilization baselines established • 2nd and 3rd years will move to performance measures • Shared Savings pool determined by both financial performance as well as quality performance
Shared Savings Model (HHS, 2011)
Data Elements for Reports • Patient identifiers (match patient across all data sources) • Patient demographics (used in patient matching algorithms) • Payer type (identify Medicare and other payer types) • Diagnoses (multiple sources, identify diabetes and comorbidities) • Lab values (discrete data from lab systems) • Blood Pressure values (documentation elements from EMRs) • Medications (from med list in EMR and pharmacy PBM) • Smoking use (documentation elements from EMRs) • Claims data (multiple sources, to track utilization)
Strategic Reports • Age distribution- Young diabetics on dialysis or with other disabilities are Medicare recipients • Gender distribution- may influence co-morbid conditions, lifestyle, compliance, choice of provider • Co-morbid conditions/Severity of illness- Patient Risk adjustment factor (RAF) score relative to the Per Member Per Month (PMPM) costs can identify gaps in care and opportunities for quality improvement • Socioeconomic status- income, education level, English proficiency impacts compliance with care/ technology ability • Patient residence- determines allocation of resources to different practice sites, likelihood of “network leakage” • Service Utilization- “network leakage”, ER utilization (appropriate and inappropriate) can identify gaps in access to care, physician referrals, and inappropriate practices
Provider Challenges • Skepticism about realized incentives relative to disruption in workflow and productivity and initial costs • No real success stories for integrated delivery systems • Need to change vital behaviors- workflow changes, evidence based algorithms, mid level providers, more granular coding, improved medical documentation to support more complex patient visit levels • Need to identify physician champions and foster a culture of communication, transparency, and teamwork • Equitability of PCP attribution- the plurality of primary care services to diabetic patients can be provided by endocrinologists • Audit tracks of individual physician performance- patient outcomes, cost
“Doctors love information; they hate to be told what to do.” Clem McDonald
Responsibilities extend well beyond the patient visit to office
Leverage the HIE for Data HIE Technical Overview (4/4/2011) from HIMSS.org
HIE Advantages • Patient centric view of information across the community for monitoring and reporting quality elements • Can use translation tables to normalize data from different sources (such as HbA1c values from different labs with different normal ranges) • Can use HL7 to bring data from multiple sources into EMRs for better use of clinical decision support at the point of care • Offer a web based portal for non-EMR providers to enter and view healthcare data • Manage referrals across community providers • Engage patients in collaborative care efforts
Financial Review ROI 1. Funding and the business case for change. ACO-like improvements require substantial investment in both time and money that may not be reimbursed directly, according to the study. While increased payments to ACOs and medical homes could create a business case for these activities, financial rewards from these investments may "not materialize for a long time, if ever.“ 2. Resistance to change. Staff members are resistant to assuming new responsibilities or delegating work they use to perform. In some cases, the organizations faced challenges in recruiting and training employees with the appropriate skills for these roles. 3. Potential disruptions to productivity. According to the study, "many of the care-delivery and infrastructure improvements [such as EMR and patient registries] required changes in workflow that affected productivity of clinical and administrative staff.4. Limited infrastructure to pursue change. Efforts to improve care coordination and delivery require a great deal of accurate data, which presents a fourth challenge to ACOs. Organizations in the study noted inaccurate data inhibits population management and financial incentives for health improvement. Organizations also mentioned concerns about sharing patient data under privacy regulations.
SUMMARY BMHA & ACO TECHNOLOGY PARTNERS • Active management of ACO participation: • Re-engineer practice workflows • Imperative: HIE link to majority of providers in region • Manage all diabetic patients with the same clinical rules • Real-time patient guidance to providers • Dashboard with practice level performance guidance • Dashboard with provider level performance/comparison
Summary of Recommendations SHORT TERM CHANGES (0- 6 MONTHS)
Short Term Changes (0-6 months) • Create monthly reporting from EHR to monitor BHMA diabetes based care quality: • Number of patients with specific chronic disease conditions of diabetes, ischemic vascular disease, hypertension, coronary artery disease, and heart failure by all payers, Medicare only, and non-Medicare • Number of patients with diabetes and have HbA1C not tested within past year, value <8%, value 8-9%, and value >9%, by all payers, Medicare and non-Medicare • Number of patients with diabetes and have BP <140/90, and =>140/90, by all payers, Medicare and non-Medicare • Number of patients with diabetes and have aspirin in their med list by all payers, Medicare and non-Medicare • Number of patients with diabetes and have LDL not tested within past year, <100 or =>100 by all payers, Medicare, and non-Medicare • Patients with a diagnosis of diabetes who have not had a visit within the previous 12 months, by all payers, Medicare and non-Medicare
Short Term Changes (0-6 months) • Create reporting from EHR to segment potential ACO patients cared for by BHMA • Number of patients with primary care visits for the group by payer, reconcile with CMS ACO reports quarterly • Create reporting from EHR to evaluate cost of care with chronic disease states: • For all patients with diabetes, those on insulin therapy with HbA1C values in the categories defined in 1. • For all patients with diabetes, medication cost estimate (using AWP for meds in patient's med list) by all payers, medicare, non-medicare • Develop Clinical Decision Support within EPIC EHR: • Alert for medications ordered but not filled within 2 weeks • Alert for laboratory tests ordered but not completed within 1 month • Alert for missed scheduled appointments for patients with diabetes • Employ a diabetes nurse navigator to review BHMA diabetes patient care reports monthly, and target resources to improve patient compliance
Summary of Recommendations MID TERM CHANGES (6-12 MONTHS)
Mid Term Changes (6-12 months) • Evaluate and select HIE vendor for functional capabilities with regards to: • Inventory of community physician participation with HIEs within the state (which physicians are connected with which HIEs) • HIE Vendor Single Sign On capability with EPIC EHR • Capture of and normalization local lab values in patient context • Capture of claims data for patient community • CCD exchange with GE Centricity for Columbia West • CCD exchange with EPIC EHR for BHMA • CCD exchange with additional community EHRs • Web Portal for direct HIE access and ability to update patient information • Disease management registry capabilities • Reporting capability for ACO patient population and BHMA patient population • Patient Portal functionality for messaging and maintaining a personal health record with updates from provider EHRs
Mid Term Changes (6-12 months) • Invest in HIE participation with priority development of the following: • Automated data exchange with EPIC EHR to retrieve HIE information upon patient visit registration and send information to HIE upon patient discharge • Bidirectional medication information exchange from HIE sources into EPIC EHR • Bidirectional lab and radiology results exchange from HIE sources into EPIC EHR • Bidirectional CCD exchange with HIE and EPIC EHR • Bidirectional messaging integration with EPIC EHR and HIE messaging for provider to provider messaging, and patient to provider messaging • Development of Clinical Decision Support tools at HIE level: • Initiate development of disease based data warehouse in HIE, with the ability to segment ACO patients as a group for reporting and alerting • Alerts to ACO and PCP for ACO concerning beneficiary utilization – such as any ED visit or hospitalization via automating messaging
Mid Term Changes (6-12 months) • Structure reports from HIE community information to evaluate ACO beneficiary utilization estimates • Define ACO patient beneficiaries within HIE patient population • For all ACO patients with diabetes number of ED encounters within past year sorted by all payers, Medicare and non-medicare • For all ACO patients with diabetes number of Ambulatory visits by specialty type sorted by all payers, Medicare and non-medicare • For all ACO patients with diabetes number of Hospital admissions sorted by all payers, Medicare and non-medicare • For all ACO patients with diabetes number of surgical procedures sorted by all payers, Medicare, and non-medicare
Mid Term Changes (6-12 months) • Structure reports from HIE community information to examine ACO diabetes care quality • Monthly list of ACO diabetes patients who have not had an HbA1C value reported within the previous 6 months reported to ACO and PCP • Monthly list of ACO diabetes patients who have not had an LDL value reported within the previous 12 months reported to ACO and PCP • Monthly list of ACO diabetes patients who have not had a Blood Pressure reading within the previous 12 months reported to ACO and PCP • Monthly list of ACO diabetes patients who have not had a primary care visit within the previous 12 months reported to ACO and PCP • Monthly list of ACO diabetes patients who have a positive tobacco use history documented reported to ACO and PCP • Summary ACO beneficiary diabetes quality measure report quarterly
Summary of Recommendations LONG TERM CHANGES (12-24 MONTHS)
Long Term Changes (12-24 months) • Revise model of diabetes care to utilize resources more effectively • Align ACO reporting to CMS to come directly from HIE, in lieu of individual group reporting on quality measures • Disease registry for ACO beneficiaries created within HIE • ACO participants send quality data to HIE via HL7 at the end of each encounter • ACO participants without EHRs can enter data directly into HIE via web portal • HIE reports quality data monthly to CMS