Download
1 / 12
120 likes | 311 Views
Mid-term results of hybrid aortic repair using a custom quadfurcated graft . Ali Khoynezhad MD, PhD, FACS, FACC Associate Professor of Cardiovascular Surgery Director of Aortic Surgery Division of Cardiothoracic Surgery Cedars-Sinai Medical Center Los Angeles, CA. Background.

E N D
Mid-term results of hybrid aortic repair using a custom quadfurcated graft Ali Khoynezhad MD, PhD, FACS, FACC Associate Professor of Cardiovascular Surgery Director of Aortic Surgery Division of Cardiothoracic Surgery Cedars-Sinai Medical Center Los Angeles, CA
Background Patients with anatomic or physiologic constrains are poor endovascular or open candidates. Hybrid repair with early promising results in this high-risk cohort Aim of this study: feasibility and midterm follow-up of hybrid aortic repairs using a custom graft Same graft can be used for hybrid arch or TAAA repair.
Why Hybrid? • Stroke risk up to 12%, • Mortality up to 20% • Proximal vs distal arch outcomes • Respiratory failure • Recurrent nerve injury • no aortic cross-clamping • Avoid second stage elephant trunk • & the interval mortality
Patient Cohort • 342 TEVARs between 2005-2011 • 195 patients requiring combined • open/endovascular approach • 52 patients with custom graft • Indications: aneurysm in 31, chronic dissection in 15, acute type A dissection in 6 • 18 (35%) had hybrid TAAA • 34 (65%) zone 0 hybrid arch repair
Comorbidities • Age 68 ±11 years (range 59-83) • 15 (29%) patients had prior aortic operation or procedure. • 12 (23%) urgent/emergent • 22 (43%) with severe COPD • 10 (19%) prior stroke/TIA • 14 (27%) with prior MI • 19 (37%) with moderate eGFR reduction (stage III CKD)
Results • In 40 (77%) patientsendovascular exclusion was performed simultaneously. • Two (4%) patients developed permanent stroke perioperatively. • No patients with spinal cord injury. • No type I or III endoleak. • No perioperative MI • 6 (12%) with acute kidney injury, no new-onset hemodialysis. • 11 (21%) atrial fibrillation
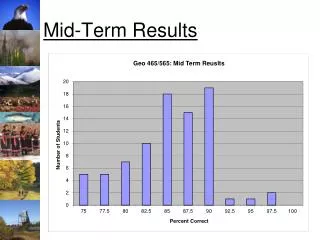
Results (cont.) • Early mortality was 6% (n=3). • 1-year and 4-year mortality were 90% & 79%
Follow-up • 51(98%) with complete follow-up. • Office visit and imaging follow-up at 1, 6, 12 months & yearly thereafter. • At a mean follow-up of 34 ± 11 months, there were six additional late deaths (none related to aorta). • All debranching bypass grafts have remained patent. • One endovascular re-intervention at 8 months.
Extra-anatomic bypass off left common iliac artery Celiac artery Superior mesenteric artery
Bypass graft to right renal artery after a small Kocher maneuver;this branch is tunneled from left to right gutter in the retroperitoneal space.
Conclusions • Hybrid aortic repair using quadfurcated graft appears to be feasible, safe and effective at mid-term follow-up. • Hybrid aortic repair represents a feasible alternative in high-risk patients. • Long-term surveillance requiring contrast administration and radiation exposure remains an unresolved issue. • Long-term results need to be established.