Download
1 / 19
200 likes | 462 Views
Spontaneous Pneumothorax In the Newborn. By: Angela Oliver-Piquette, Carly Jo Amen, Katie Kappel, & Marjerie Malabanan. Overview. During our clinical experience at St. Anthony’s North, we had the opportunity to see many births.

E N D
Spontaneous PneumothoraxIn the Newborn By: Angela Oliver-Piquette, Carly Jo Amen, Katie Kappel, & Marjerie Malabanan
Overview During our clinical experience at St. Anthony’s North, we had the opportunity to see many births. One of the most exciting was a cesarean delivery that presented with an infant who developed a spontaneous pneumothorax. Though it is rare in infants, a spontaneous pneumothorax varies from 0.07%-37.5% of all live births. We would like to take this opportunity to share with you what we learned during this clinical experience of the newborn with spontaneous pneumothorax.
Pathophysiology/Physiology • A pneumothorax is a lung disorder in which air in the lungs leaks out through a hole or holes in the lung tissue into the space between the chest wall and the outer tissue of the lungs. • Air leaks occur when the alveoli become over-distended and rupture. Some pneumothorax in infants occur spontaneously while others are due to meconium aspiration, in which the fetus inhales the first stools in utero and air becomes trapped causing over-distension.
Predisposing Factors: • Prematurity • Difficult delivery • Nucal cord • Vigorous resuscitation • Mechanical ventilation • Respiratory distress
Impact • This topic has the potential to have a huge impact on neonatal nursing, though it does not occur very frequently. • Knowing the predisposing factors and looking for those newborns at risk will ensure they receive the best, appropriate care for their condition. • Newborns suffering from some respiratory distress must be watched carefully and incorporate frequent chest radiographs if the infant’s condition declines.
Impact, conti. • Additionally, knowing the signs and symptoms of newborn respiratory distress, auscultation of lung sounds, and assessing chest expansion is imperative to the neonatal nurses who may be faced with a pneumothorax. • If nurses are educated about this topic it will ensure the best possible outcome for all neonates with respiratory distress.
Signs and Symptoms • Respiratory distress: Rapid breathing Grunting Nostril flaring Chest wall retractions
Signs and Symptoms, conti. • Sudden, unexplained deterioration in the newborn’s condition • Decreased breath sounds • Apnea • Bradycardia • Cyanosis • Increased oxygen requirements
Late Signs and Symptoms • Mottled, asymmetric chest expansion • Decreased arterial blood pressure • Shock-like appearance • Shift in the apical cardiac impulse to the side opposite the pneumothorax, often with muffled heart sounds. • Higher PCO₂ and decreased pH
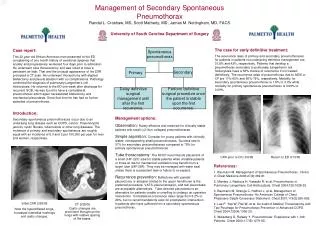
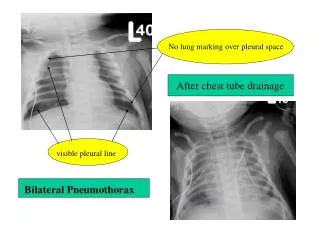
Diagnosis • X-ray examination is the major method for definitive diagnosis of pneumothorax. • Transilluminationof the chest can be performed for quick evaluation of the pneumothorax, but can be unreliable.
Treatments • Thoracentesis Hollow needle or cannula is inserted into the pleural space to release air, allowing the lung to reinflate. Because pneumothorax is potentially life-threatening for a newborn, immediate removal of accumulated air by thoracentesis may be warranted. This procedure carries a risk of damaging the lung pleura with needle tracks as the lung reinflates. *Only can be performed by specifically trained personnel*
Treatments, conti. • Chest Tube A chest tube can be inserted into the pleural space for complete resolution of the pneumothorax. *This procedure can only be performed by specifically trained personnel.*
Additional Treatments • Hood or vent • 100% Oxygen
Implications for Nursing • The most important nursing function in caring for infants susceptible to pneumothorax is close vigilance. Be alert for pneumothorax in: 1. Infants with RDS with or without positive pressure ventilation. 2. Infants with meconium-stained amniotic fluid. 3. Infants with radiographic evidence of interstitial or lobular emphysema. 4. Infants who required resuscitation at birth. 5. Infants receiving continuous positive airway pressure or positive pressure ventilation.
Implications for Nursing, conti. • Nurses working in areas where potential for this complication is high, such as newborn nurseries & NICUs, should be able to immediately recognize s/s of respiratory distress in infants. • Initial measures such as assessment of respiratory status, administration of O₂, and immediately alerting practitioners of newborn’s status. • Additionally, nurses must have needle aspiration equipment (30-ml syringe, 3-way stopcock, and 23 to 35 gauge needles) at the bedside for emergency use.
Case Study • BB, 38 wks gestation, less than one day old. • LGA, 9lbs 10oz. • Cesarean section. • Multipara • Gestational diabetes. • S/S nasal flaring, grunting, intercostal respirations, central cyanosis. • O₂ saturation consistently below 90% by SaO₂ monitor.
Treatment: • X-ray confirmation of spontaneous pneumothorax. • Humidified 100% Oxygen @ 10 liters via hood. • Created a gradient in his lungs so that air trapped in the pleural space was absorbed more effectively. • Within 5 to 6 hrs, BB was weaned down from O₂ with SaO₂ of above 92%. At approximately 8 hours, hood removed and BB able to maintain above 95% SaO₂ w/no supplemental oxygen.
References Davidson, M.R., London, M.L., & Wieland Ladewig, P.A. (2008). Maternal- newborn nursing & women’s health across the lifespan (8th ed.). New Jersey: Pearson Prentice Hall. Hockenberry, M.J. (2006). Wong’s nursing care of infants and children. (8th ed.). St. Louis: Mosby. Logan, M.D., Crispin, M.D., & Pausa, M.D. (2010). Spontaneous pneumothorax of the newborn. American College of Chest Physicians, 42, 611-614. Singh, S.A., & Amin, H. (2005). Familial spontaneous pneumothorax in neonates. Indian Journal of Pediatrics, 72, 445-447. Schneider Children’s Hospital. (n.d.). High Risk Neonate. Retrieved from http://www. schneiderchildrenshospital.org/peds_html_fixed/peds/hrnewborn/pnethorx.htm.