Download

1 / 22
230 likes | 441 Views
Pain. Types of Pain. Acute Pain Complex combination of sensory, perceptual, & emotional experiences as a result of a noxious stimulus Mediated by rapidly conducting nerve pathways & associated with increased muscle tone, heart rate, & blood pressure (sympathetic nervous system response)

E N D
Types of Pain • Acute Pain • Complex combination of sensory, perceptual, & emotional experiences as a result of a noxious stimulus • Mediated by rapidly conducting nerve pathways & associated with increased muscle tone, heart rate, & blood pressure (sympathetic nervous system response) • Intensity depends of the degree of injury • Serves as a protective function • Tx – reduce inflammation & modify transmission of pain
Types of Pain • Chronic Pain • Starts as acute pain but persists ≥ 3 – 6 months • Continues even after noxious stimulus is absent (unlike chronic inflammation) • Associated with physical (strength, endurance), psychological, & social dysfunction • Source maybe increased sympathetic response (increased sensitivity of nociceptors) or financial gain • Tx – decrease risk of chronic pain by using physical agents &/or meds to tx acute pain
Types of Pain • Chronic pain
Types of Pain • Referred Pain • Felt at one area distant from the source • Ex – spinal nerve root impingement, angina • Pain may be referred from a nerve to innervation site or from different areas of the same dermatome • Clinicians should not “chase” pain • Rule-out proximal sources of pain • Determine the structure(s) that are responsible for the pain • Rotator cuff injuries can refer pain to the lateral & upper arm • Kidney pathologies can refer pain to the low back
Specificity Theory Type of pain depends on the stimulation of specific nerve endings Pattern Theory Type of pain depends on intensity or frequency of stimulation of receptors that also respond to touch, pressure, or temperature Mechanisms of Pain Reception and Transmission
Mechanisms of Pain Reception and Transmission • Pain Receptors • Nociceptors can be activated by thermal, mechanical, or chemical stimuli
Mechanisms of Pain Reception and Transmission • Peripheral Nerve Pathways • C fibers (80%) – cause sensation of dull, throbbing, aching, or burning pain • A-delta fibers (20%) – cause sharp, stabbing, pricking pain • Both types of fibers may or may not be stimulated
Mechanisms of Pain Reception and Transmission • Pain-spasm cycle • Muscle guarding
Whiplash injury • Muscle guarding • “Protective guarding”
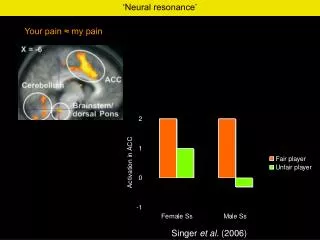
Pain Modulation and Control • Gate Control Theory • Proposed by Melzack & Wall (1965) • Degree of pain is determined by the balance of excitatory and inhibitory inputs to the spinal cord • Increased activity of the non-nociceptive fibers causes inhibition of nociceptive fibers
Pain Modulation and Control • Gate Control Theory • Physical agents and interventions “close the gate” for pain by activating nonnociceptive nerves • Ex’s – traction, compression, & massage
Pain Modulation and Control • The Endogenous Opioid System • Pain can be modulated by endogenous opioids • Opioids bind to opioids receptors in the nervous system which inhibits pain • Electrical stimulation has been shown to release endogenous opioids
Measuring Pain • Visual Analog & Numeric Scales • VAS – draw a line on the scale to indicate the present level of pain • Numeric scale – rate pain from 0-10/10 or 1 to 100 • Face Scale - Used for individuals who have difficulty understanding the VAS and numeric scales
Measuring Pain • Comparison with a Predefined Stimulus • May allow greater intrasubject & intersubject reliability • The subject compares the present pain to a predefined stimulus • Tourniquet pain, electrical pain, thermal pain, or pressure pain • You can imagine the limitations to this form of assessment!!!
Measuring Pain • Semantic Differential Scales • Consists of word lists and categories that represent various aspects of pain • McGill pain questionnaire • Attempts to quantify pain
Measuring Pain • Other Measures • Daily activity/pain logs • Body diagrams • Open-ended, structured interviews • Pain response to examination tests/measures
Pain Management Approaches • Pharmacological Approaches • Systemic Analgesics • Non-steroidal anti-inflammatory drugs (NSAIDS) • Acetaminophen • Opiates • Antidepressants • Spinal Analgesia • Local Injection
Pain Management Approaches • Physical Agents • Cryotherapy – reduce local metabolism & slow production of histamine, bradykinin, & prostaglandins • Cryotherapy, thermotherapy, & traction stimulate non-nociceptive nerve fibers • Physical agents have some advantages over medications • Ex – less side-effects and can be readily used by the patient (ice pack or hot pack)
Pain Management Approaches • Multidisciplinary Pain Treatment Programs • Teams consist of the patient, families, PTs, MDs, RNs, psychologists, etc • Management techniques include: medications, physical agents, therapeutic exercise, &/or psychological intervention • Pain Clinics