Download
1 / 63
821 likes | 2.08k Views
Achilles Tendon Injuries. Johan Myburgh September 2011. Hippocrates. “ this tendon if bruised or cut, causes the most acute fevers, induces choking, deranges the mind and at length brings death. ”. PATIENT. 31 year old male R ecreational soccer player W ork - oilfield worker

E N D
Achilles Tendon Injuries Johan Myburgh September 2011
Hippocrates “this tendon if bruised or cut, causes the most acute fevers, induces choking, deranges the mind and at length brings death.”
PATIENT • 31 year old male • Recreational soccer player • Work - oilfield worker • Healthy - no significant past hx • Played varsity soccer and football till 23 years old
Injury • Came directly from work , no warm up • Previous tightness and tenderness calf few days • 5 minutes into game: Pushed off back to leg drive forward Sudden pain and weakness left leg
3 Stage Assessment 1. Clinical: • 80% acute partial Achilles tendon rupture • Previous sprain of Triceps surea • Improper warm up before activity
3 stage assessment 2. Personal: • concerned about the amount of time he is going to loose at work- no income. • positive about the outcome and wants to do proper rehabilitation to speed up his recovery 3. Contextual: • manager at work is supportive • seasonal work - needs to recover before the work season is over. • family is very supportive.
Treatment • Nonoperative treatment plan • Immobilized equinis cast for 7 weeks • Removable walking splint for 6 weeks • Patient did 3 weeks • Physiotherapy starting at week 7 Progression: Week 13 physical exam: • Dorsiflexion L 96° R 105° • Tendon thickness L 30 mm R 19 mm
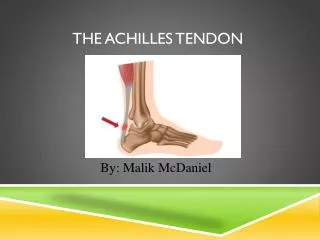
Anatomy • Formed by tendinous portion of gastrocnemius and soleus ( contribution varies) • Progresses from round to flat distally to insert on calcaneal tuberosity • Distal rotational twist (90°) • gastrocnemius fibers insert lateral • soleus fibers insert medial • Plantaris lies medial - distinct tendon (absent 6-8%) • No synovial sheath – wrapped paratenon
Blood Supply • Posterior tibialartery - majority of the blood supply • Musculotendinous junction • Bone-tendon junction • Peroneal artery • Surrounding connective tissue (paratenon/mesotenon) Poor vascularization in midportion of tendon • Angiographic and histological techniques showed Achilles tendon has a poor blood supply throughout its length = small number of blood vessels per cross-sectional area(1,4)
Histology • Fibroblasts (Embedded in bundles of fibrils) • Collagen comprises 70% of tendon • 95% type I • Ruptured tendon contains significant type III collagen • Collagen of granulation tissue - produced quickly by young fibroblasts before tougher type I collagen is synthesized Wavy bundles collagen
Histology • Collagen organized into • parallel bundles of fibrils • Surrounded by endotenon • Units surrounded by • vascular epitenon
Pathology Achilles tendon disorders and overuse injuries: • Inflammation of the peritendinous tissue (peritendinitis,paratendinitis) • Degeneration of the tendon (tendinosis) • Tendon rupture • Partial/Complete • Acute/Chronic • Insertionaldisorders (retrocalcaneal bursitis and insertionaltendinopathy)
Tendinosis Degeneration with no significant inflammation: • Hypoxic or fibromatous: • most frequently seen in ruptured tendons • Myxoid • 2nd most common • May be silent prior to rupture • Lipoid • Age dependent fatty deposits that do not affect structural properties • Calcific • Calcium pyrophosphate
General Decreased perfusion Hyperthermia within relatively avascular Achilles tendon – more prone rupture Systemic diseases Inflammatory and autoimmune conditions Collagen disorders Infectious disease Neurologic conditions Age >30 Decrease in maximum diameter & density of collagen fibrils Etiology – Intrinsic Factors
General Corticosteroids Corticosteroid injection into rabbit tendons showed necrosis and delayed healing. Several studies showed collagen damage with injected steroids. Oral steroids also implicated(2) Fluoroquinolone(3) Etiology – Extrinsic factors
Biomechanical factors Rapid push off Tendon obliquely loaded, muscle maximum contraction and initial short tendon length Functional / Anatomical conditions Imbalance agonist muscle contractions(7) Functional overpronation on heel strike (midfoot) – whipping action on Achilles – intratendinous microtears Poor flexibility gastroc/soleus - overpronation Etiology – Extrinsic factors
Biomechanical factors Unequal tensile forces of different parts tendon - torsional ischemic affect (transient vasoconstriction of intratendinous vessels, contribute vascular impairment already present) Malfunction/Suppression of proprioceptive component of skeletal muscle (athletes resume training after period rest) Etiology – Extrinsic factors
Epidemiology • Incidence increasing significantly • 8.3 ruptures per 100 000 people(18) • Gender • Males 2:1 over females • Age (two peaks) • 30-50 – sports activity-related • > 50 – non-athletes and women • Sport • abrupt repetitive jumping • sprinting movements • Race - increased African-Americans(8)
Histology of Rupture • Collagen degeneration of tendonprior to rupture(4) • Marked inflammatory reaction • Hypertrophy of tunica media and narrowing of lumen of large peritendinousvessels(1) - hypoxia All based on biopsy at time of surgical repair
Site of Rupture • MyotendinousJunction • Midsubstance2-6 cm proximal • to insertion • Hypovascular • Avulsion
Diagnosis History Male between 30 and 50 years Sedentary job but in athletic activity “Weekend Warrior” Pop, “kicked”in the back of the leg Pain posteriorly in calf. Pain is variable Bruising
Diagnosis Clinical dx Physical: Palpable defect Thompson Test Single leg heel raise Bruising/Swelling Weakness
Thompson Test Patient prone with feet dangling - squeeze mid calf NO plantar flexion = positive Thompson test /Ruptured tendon
Diagnosis • Diagnostic Tests • Ultrasound (Doubtful cases) • Helpful with Non-operative treatment Used to assess gap in tendon and apposition of torn ends of tendon • MRI (not routinely) • Show extent of tendon degeneration • X-rays • Avulsion of calcaneus suspected
Ultrasound = Hematoma in Achilles tendon Most widely used U.K + Inexpensive Readily available, fast Dynamicassessment Tendon thickness Gap // torn ends − Operator dependent Miss partial tears
MRI Most widely used imaging U.S +Accurate Partial tears − Not readily available High cost No dynamic assessment
Nonoperative Treatment Effective for all age groups and both sedentary and sporting individuals • Wide variability among surgeons • absolute immobilization • initial range of movement exercises • progression weight bearing status • Cast immobilization 4-8 week (non-weight bearing) • Functional brace 4-6 weeks • Use ultrasound to ensure tendon apposition
Nonoperative Treatment • Higher rerupture rate (13%) vs. operative repair (4-5%)(10) • Fewer overall complications ( wound infection) • Complications may be reduced with percutaneous surgery
Surgical treatmentTwo Decisions Surgical technique Postoperative regime
Surgical Technique • Direct Open (Incision 10-18 cm) • Mini-invasive (Incision 3-10 cm) • Percutaneous (multiple small incisions)
Percutaneous Achilles Repair • vs. Open repair: • Higher rerupture rate (6.4% vs 2.7%) • Fewer complications • Allow earlier mobilization • Earlier functional rehabilitation • Sural nerve entrapment
Open Repair Postero-medial incision Incision site reduce risk injury sural nerve and branches. Easier access plantaris muscle
Percutaneous Repair Achillon Device
Complications of Surgical Treatment • Wound healing problems/necrosis • Wound infection • Sural nerve injury • DVT and PE • Rerupture 2-5%
Chronic Rupture Definition: 4-6 weeks from time of injury to diagnosis and treatment • Conservative management not recommended • Fibrous tissue in gap between torn ends • Poor plantar flexion strength (2° flexors foot) • Open repair and reconstruction
Postoperative Regime • Consensus Early functional weight bearing and range of motion decrease: Inpatient stay Time off from work Faster return to sport Lower complication rate • No Consensus DVT prophylaxis DVT common after Achilles tendon rupture No evidence to demonstrate benefit • Start ROM exercises Day 10 / earlier as per pt’s comfort • Day 14 weight bearing with restricted dorsiflexion