Download
1 / 60
600 likes | 776 Views
HUMAN IMMUNODEFICIENCY VIRUS Maternal-Fetal Presentation. Socorro Quimson, SNNP The University of Texas Medical Branch School Of Nursing NNP I GNRS 5631 Leigh Ann Cates PhD, APRN, NNP-BC, RRT-NPS,CHSE Debra Armentrout , PhD, RN, NNP-BC. OBJECTIVEs.

E N D
HUMAN IMMUNODEFICIENCY VIRUS Maternal-Fetal Presentation Socorro Quimson, SNNP The University of Texas Medical Branch School Of Nursing NNP I GNRS 5631 Leigh Ann Cates PhD, APRN, NNP-BC, RRT-NPS,CHSE Debra Armentrout, PhD, RN, NNP-BC
Review HIV epidemiology, Maternal and Fetal pathophysiology and impact of maternal condition to the fetus. • Examine the maternal and fetal clinical manifestation and its therapeutic approaches and treatment options. • Discuss pertinent theories and evidence based practice and its economic, emotional and social implication on the family unit. OBJECTIVEs
The Joint United Nations Program on HIV/AIDS (UNAIDS) reports that new HIV infections have been on the rise in Eastern Europe and Central Asia by 13% since 2006. The Middle East and North Africa has seen a doubling of new HIV infections since 2001. • In 2012 an estimated 35.3 million of people globally were living with HIV, 2.3 million of people became infected of HIV and 1.6 million people died of AIDS related illness. In. 2011, an estimated 49,273 people were diagnosed with HIV infection in the United States. (CDC, 2013, p. 1). (UNAIDS, 2013, p. 1) ePIDEMIOLOGY
In 2010, an estimated 1.49 million (1.3–1.6 million) pregnant women in low- and middle-income countries were living with the human immunodeficiency virus (HIV). Each year, many children are newly infected with HIV, mainly through maternal and fetal transmission. Without help, most of these children will die by their second birthday. (United Nations International Children’s Emergency Fund [UNICEF], 2012, p. 1) EPIDEMIOLOGY
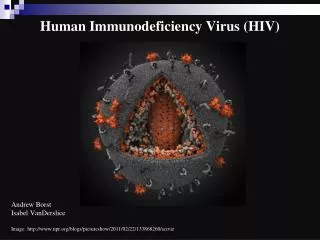
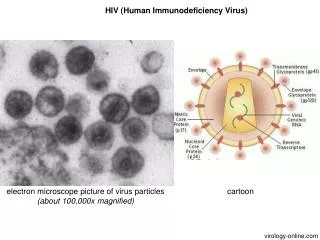
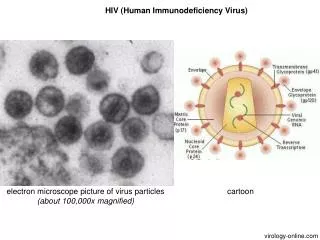
HIV is a blood-borne virus Member of the retrovirus family, which carries genetic information in the form of two copies of RNA. Retrovirus use a viral enzyme, reverse transcriptase, to convert RNA into double-stranded DNA (Rote & Huether, 2010, p. 319). Human immunodeficiency virus pathophysiology
New DNA is inserted into the infected cell’s genetic material If the cell is activated, translation of the viral information may be initiated Formation of new virions, lysis, and death of the infected cell, and shedding of infectious HIV particles. (Rote & Huether, 2010, p. 319). Human immunodeficiency virus pathophysiology
HIV actively replicates in lymph nodes and circulating CD4+ cells Profound disruption of the immune system The host is placed at risk for acquiring infections with organisms that normally possess low pathogenicity (Baley & Toltzis, 2011, p. 860). HUMAN IMMUNODEFICIENCY VIRUS pathophysiology
Maternal HIV pathophysiology (Rote & Huether, 2010, p. 319-322)
HIV infection of the fetus and even in full term newborns results in particularly severe disease because: • Natural Killer and T cells are low in number and immature in function ( Fetus). • T cells possess multiple functional deficiencies ( Full Term Newborns ). • Sluggish or absent Early HIV-specific cytotoxic T cell lymphocyte responses. (Baley & Toltzis, 2011, p. 860). fetal HIV pathophysiology
Maternal to Fetal or Neonatal Transmission • Antepartum(before onset of labor) • Peripartum (during labor & delivery)- highest risk • Breastfeeding- predominant means of postnatal HIV transmission (Schleiss & Patterson, 2012, p. 506) Maternal & fetal pathophysiology
The outcome of pregnancy can be adversely affected by maternal HIV infection even if the infant is not infected. Studies in Africa have shown that infants of women ill with HIV infection are smaller for gestational age, and are more premature compared with infants of women without HIV infection. Perinatal mortality also is increased. (Baley & Toltzis, 2011, p. 860). Impact of the maternal condition to the fetus
Studies have illustrated that infants born to asymptomatically infected women have negligible effects. These data suggests that factors covariate with advance HIV disease, particularly malnutrition, secondary and coexisting infections, and illicit drug and alcohol use , are the most important factors mediating the immediate health of the newborn and must be addressed appropriately during the obstetric care of the mother (Baley & Toltzis, 2011, p. 860). Impact of the maternal condition to the fetus
CLINICAL MANIFESTATION & DIAGNOSTIC EVALUATION OF THE NEONATE
Neonatal Signs and Symptoms: • Mostly asymptomatic • Low birth weight • Failure to thrive (if infected in utero). • Herpes zoster, disseminated • Mycobacterium avium complex (MAC), Pneumocystis Pneumonia (PCP), and • candidiasis • Hepatosplenomegaly, • Lymphadenopathy • Fever. • (Gomella, 2009, p. 472) Clinical manifestations OF THE NEONATE
Common CT scan findings include basal ganglia calcification and cortical atrophy. Cardiac abnormalities including pericardial disease, myocardial dysfunction, dysrthythmias, and cardiomyopathies are common, particularly in advanced disease. (Gomella, 2009, p. 472). Clinical manifestations OF THE NEONATE
Maternal Screening • Enzyme-Linked ImmunosorbentAssay (ELISA) • Western Blot • Blood Counts and Viral load • Hepatitis Testing • Opportunistic infection Assessment • Other sexually transmitted disease • Vaccination • Tuberculosis Testing • Presentation during Labor (Marino, 2012, p. 1) Maternal diagnostic evaluation
NEONATAL ( younger than 18 months of age) DIAGNOSTIC EVALUATION • HIV Serology Or Antibody Tests (ELISA, Western Blot) Screens HIV Exposure, not reliable for diagnosing HIV infection • Virologic Assays (HIV-1 DNA and RNA PCR) Screens HIV infection • Rapid Test detects IgG antibodies against HIV • Surrogate markers for disease Hypergammaglobulinemia, low CD4 T-lymphocyte count or a decreased CD4 percentage (Gomella, 2009, p. 473-474) DIAGNOSTIC EVALUATION OF THE NEONATE
NEONATAL ( younger than 18 months of age) DIAGNOSTIC EVALUATION • HIV-1 DNA and RNA polymerase chain reaction (PCR) is the gold standard for diagnosis of HIV in infants and children less than 18 months. • TheHIV-1 DNA PCR assay as the preferred diagnostic tool. A positive results identifies infants who were infected in utero. • Among those infants who test positive, a CONFIRMATORY TEST on a new sample should be performed but antiretroviral therapy should not be delayed while awaiting results. (WHO, 2014, p. 20) Diagnostic evaluation of the neonate
NEONATAL ( younger than 18 months of age) DIAGNOSTIC EVALUATION • In a situation where symptoms exist, serological test is positive,and virological testing is unavailable, treatment may be initiated in the bases of presumptive clinical diagnosis • Treatment should not be denied to infants with severe manifestations of HIV infection even though their diagnosis has not been confirmed (University of California, San Francisco [UCSF], 2014, Module 2) Diagnostic evaluation of the neonate
The major part of the management of HIV infection is antiretroviral therapy. This should be offered to all symptomatic patients regardless of CD4 cell count. At present, there is no cure for HIV infection, but the goal of antiretroviral therapy is to suppress the HIV viral load and to maintain or reconstitute CD4 cell numbers to greater than 25%. (Burchett, 2012, p. 608). Therapeutic approaches & treatment options
Four classes of Antiretroviral drugs • Nucleoside or Nucleotide analog reverse transcriptase inhibitors (NRTI). Example: Zidovudine(AZT). • Non-Nucleoside analog reverse transcriptase inhibitors (NNRTIs). Example: Niveripine • Protease Inhibitors (PIs) • IntegraseInhibitors (Burchett, 2012, p. 608). Therapeutic approaches & Treatment options
Infant Antiretroviral Prophylaxis recommendation in the United States • The 6-week neonatal component of the zidovudine chemoprophylaxis regimen is recommended for all HIV-exposed neonates to reduce perinatal transmission of HIV. 1 • Zidovudine, at gestational age-appropriate doses, should be initiated as close to the time of birth as possible, preferably within 6 to 12 hours of delivery. (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 167). Therapeutic approaches & treatment options
Infant Antiretroviral Prophylaxis recommendation in the United States • Infants born to HIV-infected women who have not received antepartum antiretroviral drugs should receive prophylaxis with ZIDOVUDINE given for 6 weeks combined with three doses of NEVIRAPINE in the first week of life (first dose at birth, 48 hours later, and 96 hours after the second dose), begun as soon after birth as possible. (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 167). Therapeutic approaches & treatment options
Infant Antiretroviral Prophylaxis recommendation in the United States • In the United States, the use of antiretroviral drugs other than Zidovudine and Nevirapinecannot be recommended in premature infants because of lack of dosing and safety data. (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 167). Therapeutic approaches & treatment options
Infant Antiretroviral Prophylaxis in the United States • In other scenarios, the decision to combine other drugs with the 6-week ZIDOVUDINE regimen should be made in consultation with a pediatric HIV specialist, preferably before delivery, and should be accompanied by counseling of the mother on the potential risks and benefits of this approach. (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 167). Therapeutic approaches & treatment options
Recommended Neonatal Dosing for Prevention of Mother-to-Child Transmission of HIV (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 172)
Recommended Neonatal Dosing for Prevention of Mother-to-Child Transmission of HIV (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 172)
Recommended Neonatal Dosing for Prevention of Mother-to-Child Transmission of HIV (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 172)
Recommended Neonatal Dosing for Prevention of Mother-to-Child Transmission of HIV Additional Antiretroviral Prophylaxis Agentfor HIV-Exposed Infants of Women who Received No Antepartum Antiretroviral Prophylaxis(initiated as soon after delivery as possible) (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 172)
Side Effects of Antiretroviral Therapy Exposure in infants • Studies have shown an increase risk of prematurity and very low birth weight in infants born to mothers receiving antiretroviral therapy regimens containing a protease-inhibitor drug. In addition anemia, hypersensitivity reaction, thrombocytopenia, neutropenia and decreased level of lymphocytes have been identified among infants exposed to antiretroviral therapy. (Schleiss& Patterson, 2012, p. 511) Therapeutic approaches & treatment options
Recommendation for Initial Postnatal Management of the HIV-Exposed Neonate in the United States • Hemoglobin and neutrophil counts 4 weeks after initiation of prophylaxis for infants who receive combination zidovudine/lamivudine-containing antiretroviral prophylaxis regimens. • Virologic Tests should be performed within the first 14 to 21 days of life, at 1 to 2 months, and at 4 to 6 months of age. (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 179) (Schleiss & Patterson, 2012, p. 511) Therapeutic approaches & treatment options
Recommendation for Initial Postnatal Management of the HIV-Exposed Neonate in the United States • Baseline CBC with differential • Hematologic and serum chemistry and liver function assays at birth and when diagnostic HIV PCR tests are obtained in infants exposed to combination antiretroviral drug regimens in utero orduring the neonatal period (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 179) Therapeutic approaches & treatment options
Recommendation for Initial Postnatal Management of the HIV-Exposed Neonate in the United States • Trimethoprim-sulfamethoxazole(Co-trimoxazole) prophylaxis at age 4- 6 weeks to prevent Pneumocystis jiroveciipneumonia to all infants born to women with HIV infection • Dosage: 75 mg per dose, twice a day , 3 days a week (Baley & Toltzis, 2011, p. 865) (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 179).3 Therapeutic approaches & treatment options
Recommended Initial Postnatal Management of the HIV-Exposed Neonate in the United States • Health care providers should routinely inquire about PREMASTICATIONof foods fed to infants, instruct HIV-infected caregivers to avoid this practice, and advised on safer feeding options (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 179) Therapeutic approaches & treatment options
Maternal Therapeutic approach • All pregnant and breastfeeding women with HIV should initiate triple antiretroviral drugs, which should be maintained at least for the duration of mother-to-child transmission risk. (World Health Organization [WHO], 2013, p. 100). Therapeutic approaches & treatment options
Maternal Therapeutic approach • A once-daily fixed-dose combination of TenofovirDisoproxilFumarate(TDF) + lamivudine (3TC) or Emtricitabine (or FTC) + Efavirenz (EFV) is recommended as first-line antriretroviral therapy in pregnant and breastfeeding women, including pregnant women in the first trimester of pregnancy and women of childbearing age. (World Health Organization [WHO], 2013, p. 30). Therapeutic approaches & treatment options
INFANT FEEDING • In 2010, WHO recommended that ANTIRETROVIRAL DRUGS be provided either to the mother or the infant throughout breastfeeding to reduce the risk of postnatal HIV transmission. • Colostrum viral load is particularly high • In the USA it is recommended to AVOID BREASTFEEDING (Schleiss & Patterson, 2012, p. 509) (WHO, 2013, p. 105) (Gomella, 2009, p. 472) Pertinent theories & evidence based practice
VACCINE • Inactivated Vaccine can be administered safely • Routine immunization schedules fro DaTP, IPV , Hib, HBV, hepatitis A vaccine, and PCV. • Annual influenza vaccine. • Live vaccine such as MMR and Varicella ( can be given at 12 months of age if not severely immunosuppressed). (Centers for disease control and prevention Atlanta, GA, 2013, p. 1) (Gomella, 2009, p. 472) Pertinent theories & evidence based practice
Perinatal Transmission of HIV and Maternal HIV RNA Copy Number • Because transmission can occur even when HIV RNA copy numbers are low or undetectable, all HIV- infected women should be counseled about and administered antiretroviral drugs during pregnancy, regardless of their HIV RNA levels. (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 19) Pertinent theories & evidence based practice
International Clinical Trials of Short-Course Antiretroviral Regimens for Prevention of Perinatal Transmission of HIV. • Combination of infant antiretroviral prophylaxis is recommended in the United States for infants whose mothers have not received antenatal antiretroviral drugs. Multi country clinical trial demonstrated that the combination regimens reduced risk of intrapartum transmission by approximately 50% compared with infant prophylaxis with zidovudinealone. (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 22). Pertinent theories & evidence based practice
When to start antiretroviral therapy • Early treatment initiation is associated with clinical and HIV prevention benefits, improving survival and reducing the incidence of HIV infection at the community level. The 2013 WHO Guidelines Development Group recommends to initiate antiretroviral therapy in all pregnant and breastfeeding women with HIV, all children younger than five years living with HIV and all individuals with HIV in serodiscordant relationships, regardless of CD4 cell count (WHO, 2013, p. 92). Pertinent theories & evidence based practice
HIV Testing and Counselling • It is recommended that provider will initiate testing and counselling in routine infant care settings for additional case finding. Provider-initiated testing and counselling is particularly recommended for all children who are malnourished, have TB, are admitted to hospital or have other signs or symptoms of HIV infection (WHO, 2014, p. 20) Pertinent theories & evidence based practice
Delivery Method • The current ACOG recommendations, updated in December 2010, recommend that all HIV–positive pregnant women with plasma viral loads greater than 1000 copies per milliliter be “counseled regarding the benefits of an elective cesarean delivery” in addition to a zidovudine infusion 3 hours before the operation. • Viral loads of < 1000 copies /ml ( No benefits of cesarean delivery, women should be informed) (Schleiss& Patterson, 2012, p. 509) (Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission, 2012, p. 152) Pertinent theories & evidence based practice
Viral load Monitoring • Viral load is recommended as the preferred monitoring approach to diagnose and confirm ARV treatment failure in adults, adolescents and children. If viral load is not routinely available, CD4 count and clinical monitoring should be used to diagnose treatment failure (WHO, 2013, p. 133). Pertinent theories & evidence based practice