Download

1 / 36
650 likes | 1.57k Views
Hyponatremia Dr. Kavitha Ramaswamy, Department of Internal Medicine August 11, 2009 1. The Definition of Hyponatremia Normal serum sodium level : 135 – 145mEq/L Hyponatremia is defined as a serum sodium level less than 135mEq/L

E N D
Hyponatremia Dr. Kavitha Ramaswamy, Department of Internal Medicine August 11, 2009
1. The Definition of Hyponatremia • Normal serum sodium level : 135 – 145mEq/L • Hyponatremia is defined as a serum sodium level less than 135mEq/L • Considered severe when the serum level is less than 120mEq/L
2. Pathophysiology • Generally, hyponatremia is of clinical significance only when it reflects a drop in the serum osmolality • Hypoosmolality (serum osmolality<280mOsm/kg) Excess total body water relative to body solutes : Due to solute depletion, solute dilution, or a combination of both.
In the normal condition • Renal handling of water is sufficient to excrete as much as 15-20 L of free water per day. • The body's response to a decreased osmolality is decreased thirst. Therefore, hyponatremia is the result of • Impairment of normal free water excretion and/or • Impairment of the normal thirst mechanism
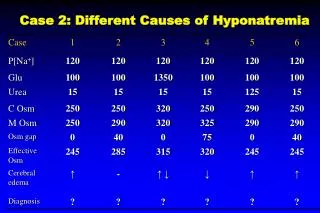
3. Causes of Hyponatremia Serum osmolality = 2x[Na+](mEq/L) + serum glucose(mg/dL)/18 + BUN (mg/dL)/2.8 (or it can be measured directly via osmometry) • Pseudohyponatremia • Normal plasma osmolality • Increased plasma osmolality II. Hypoosmolal hyponatremia
Pseudohyponatremia • Normal plasma osmolality • Hyperlipidemia • Hyperproteinemia • Posttransurethral resection of prostate/bladder tumor • Increased plasma osmolality • Hyperglycemia • Mannitol
Hypoosmolal hyponatremia • Primary Na+ loss (secondary water gain) • Integumentary loss: sweating, burns • Gastrointestinal loss: vomiting, diarrhea • Renal loss: diuretics, osmotic diuresis, hypoaldosteronism, salt-wasting nephropathy
B. Primary water gain(secondary Na+ loss) • Primary polydipsia • Decreased solute intake • AVP release due to pain nausea, drugs • SIADH • Hypothyroidism • Chronic renal insufficiency C. Primary Na+ gain (exceeded by secondary water gain) • Heart failure • Hepatic cirrhosis • Nephrotic syndrome
Causes of Hypotonic Hyponatremia Adrogue H and Madias N. N Engl J Med 2000;342:1581-1589
4. Diagnosis • Hyponatremia is not a disease but a manifestation of a variety of disorders. • Underlying cause can often be ascertained from: • Accurate history • Physical examination • Assessment of ECF volume status and effective circulating volume • Laboratory findings
History • Patients may develop clinical symptoms due to the cause of hyponatremia or the hyponatremia itself. • Many patients present due to manifestations of other medical comorbidities, with hyponatremia only being recognized secondarily. For many people, the recognition is entirely incidental. • Many medical illnesses, such as congestive heart failure, liver failure, renal failure, or pneumonia, may be associated with hyponatremia. These patients frequently present because of primary disease symptomatology (e.g., dyspnea, jaundice, uremia, cough).
Symptoms due to hyponatremia itself are related to osmotic water shift leading to increased ICF volume • Specifically brain cell swelling or cerebral edema • Therefore, the symptoms are primarily neurologic. • The severity is dependent on the rapidity of onset and absolute decrease in plasma Na+ concentration. • A gradual drop of the serum sodium, even to very low levels, may be tolerated well if it occurs over several days to weeks because of neuronal adaptation.
Effects of Hyponatremia on the Brain and Adaptive Responses Adrogue H and Madias N. N Engl J Med 2000;342:1581-1589
Asymptomatic or Nausea and malaise Headache Lethargy Confusion Obtundation Stupor Seizures Coma Acute decrease in Na+ level below 120mEq/L or Rapid decrease(<72hr)
A Detailed medication history (including over-the- counter (OTC) drugs) is important • Many medication may precipitate hyponatremia (eg, antipsychotic medications). • Diuretic-induced hyponatremia is almost always due to thiazide diuretics. • A dietary history with reference to salt and water intake is useful as well. • For patients who are hospitalized, reviewing the records of parenteral fluids administered is crucial.
Physical Examination • Examination should include orthostatic vital signs and an accurate assessment of volume status. This determination (ie, hypervolemic, euvolemic, hypovolemic) often guides treatment decisions. • A full assessment for medical comorbidity also is essential, with particular attention paid to cardiopulmonary and neurologic components of the examination.
Laboratory findings Three useful laboratory findings • The plasma osmolality • The urine osmolality • The urine Na+ concentration
The goals of therapy To raise the plasma Na+ concentration by restricting water intake and promoting water loss To correct the underlying disorder 5. Treatment
Hypoosmotic hyponatremia Guide treatment by the 3 following factors: • Patient's volume status • Duration and magnitude of the hyponatremia • Degree and severity of clinical symptoms
Hypovolemic hyponatremia • Administer isotonic saline Restoration of euvolemia removes the hemodynamic stimulus for AVP release Excretion of the excess free water
Hypervolemic hyponatremia • Reflect the severity of the underlying disease • Usually asymptomatic • Increased total body water that exceeds the increase in total body Na+ Treatment is • Restriction of Na+ and water intake • Correction of hypokalemia • Promotion of water loss in excess of Na+ • Correction of underlying disorder
Euvolemic hyponatremia • Water restriction • Patients who are asymptomatic, and mildly hyponatremic Free water restriction (1 L/d) is generally the treatment of choice. • Base the volume of restriction on the patient's renal diluting capacity. • Pharmacological agents • Can be used in some cases of more refractory SIADH • Allow more liberal fluid intake. • Demeclocycline is the drug of choice • Increase the diluting capacity of the kidneys by achieving vasopressin antagonism and a functional diabetes insipidus.
Rate of correction of hyponatremia • Depends on the absence or presence of neurologic dysfunction • Related to the rapidity of onset and magnitude of the fall in plasma Na+ concentration • In asymptomatic patients • No more than 0.5 to 1.0mmol/L per h • Less than 10 to 12mmol/L over first 24h
Acute or severe hyponatremia (plasma Na+ concentration<110 to 115mmol/L) • Use hypertonic saline • 1 to 2mmol/L per h for the first 3 to 4 h or Until the seizures subside • Less than 10 to 12mmol/L over first 24h
Formulas for Use in Managing Hyponatremia and Characteristics of Infusates Adrogue H and Madias N. N Engl J Med 2000;342:1581-1589
Example 1 • 32-year-old woman has three grand mal seizures two days after an appendectomy. She receives 20 mg of diazepam and 250 mg of phenytoin intravenously and undergoes laryngeal intubation with mechanical ventilation. Three liters of 5 percent dextrose in water had been infused during the first day after surgery, and the patient subsequently drank an unknown but substantial amount of water. Clinically, she is euvolemic, and she weighs 46 kg. She is stuporous and responds to pain but not to commands. The Na concentration is 112 mmol per liter, the K concentration is 4.1 mmol per liter, serum osmolality is 228 mOsm per kilogram of water, and urine osmolality is 510 mOsm per kilogram of water.
Solution • According to formula 1 of the table, 1 liter of 3 % sodium chloride will increase the serum sodium conc by 16.7 mmol/liter • (513-112/23+1=16.7 • The initial goal is to raise the serum sodium conc by 3 mmol/liter over the next three hours; thus, 0.18 liter of hypertonic sodium chloride , or 60 ml per hour is required.
Example 2 • A 58-year-old man with small-cell lung carcinoma presents with severe confusion and lethargy. Clinically, he is euvolemic, and he weighs 60 kg. The serum sodium concentration is 108 mmol per liter, the serum potassium concentration is 3.9 mmol per liter, serum osmolality is 220 mOsm per kilogram of water, the serum urea nitrogen concentration is 5 mg per deciliter (1.8 mmol per liter), the serum creatinine concentration is 0.5 mg per deciliter (44.2 µmol per liter), and urine osmolality is 600 mOsm per kilogram of water
Solution • According to formula 1 of the table, the retention of 1 liter of 3 percent sodium chloride will increase the serum sodium conc by 10.9 mmol per liter(513-108)/36+1= 10.9 • If the initial goal is to increase the serum sodium conc by 5 mmol per liter over next 12 hours, then 0.46 liter of 3 %sodium chloride (5/10.9), or 38 ml per hour is required.
Example 3 • A 68-year-old woman is brought to the hospital because of progressive drowsiness and syncope. She is being treated with a low-sodium diet and 25 mg of hydrochlorothiazide daily for essential hypertension; she has had diarrhea for the past three days. She is lethargic but has no focal neurologic deficits. She weighs 60 kg. Her blood pressure while in a supine position is 96/56 mm Hg, and the pulse is 110 beats per minute. The jugular veins are flat, and skin turgor is decreased. The serum sodium concentration is 106 mmol per liter, the serum potassium concentration is 2.2 mmol per liter, the serum bicarbonate concentration is 26 mmol per liter, the serum urea nitrogen concentration is 46 mg per deciliter (16.4 mmol per lt, the serum creatinine concentration is 1.4 mg per deciliter (123.8 µ mol per liter), serum osmolality is 232 mOsm per kilogram of water, and urine osmolality is 650 mOsm per kilogram of water
Solution • According to formula 2 of table 2, retention of 1 liter of infusate will increase the serum sodium conc by 2.8 mmol per liter (154+30-106)/27+1=2.8
Questions from MKSAP • A 73-year-old woman is brought to the emergency department after falling at home. Her family states that she has been very confused and disoriented over the past 2 days and that she began therapy with a new medication 1 week ago. She also has type 2 diabetes mellitus. • On physical examination, temperature is 37 °C (98.6 °F), pulse rate is 68/min, respiratory rate is 12/min, and blood pressure is 115/65 mm Hg. She is confused and unable to appropriately answer questions. Cardiac examination is normal. The lungs are clear to auscultation. There is no edema. • Glucose 94, BUN 17, Creatinine 1.1, sodium 107, potassium 2.9, chloride 76, bicarbonate 21. Which agents are most likely recently started in this patient Furosemide Acetazolamide Spironolactone HCTZ
A 34-year-old woman who underwent elective laparoscopic bilateral tubal ligation 1 day ago develops severe headache and nausea the next morning. During the surgery, 5% dextrose in ¼ strength normal saline therapy is initiated and maintained at 125 mL/h. She remains in recovery until late in the afternoon because she is too sedated to be discharged. Intravenous meperidine is administered with adequate relief of her pain. • Glucose 115, BUN 12, Creatinine 1.0, sodium 126, potassium 3.9, chloride 96, bicarbonate 22. • What is the next step?
References • Uptodate online • Hyponatremia: Horacio J. Adrogue, M.D., and Nicolaos E. Madias, M.D, New England Journal of Medicine • Medical knowledge self assessement program 14