Download

1 / 72
1.47k likes | 3.1k Views
Hyponatremia. Osmolality vs Effective Osmolality. Osmolality : total number of particles in an aqueous solution (mosmol/kg H2O) Normal Posm = 275-290 mosmol/kg

E N D
Osmolalityvs Effective Osmolality • Osmolality: total number of particles in an aqueous solution (mosmol/kg H2O) • Normal Posm = 275-290 mosmol/kg • Effective osmolality (tonicity): those particles that can exert osmotic force across membranes, via movement of water into or out of cells • Examples: Na+, glucose, mannitol • Normal effective Posm = 270-285 mosmol/kg
Plasma Osmolality • Na+, glucose and BUN are major determinants of plasma osmolality • Posm = 2 x plasma [Na+] + [Glucose]/18 + [BUN]/2.8 • More important clinically to consider effective osmolality than “total’’ osmolality • Effective osmoles (Na+ , glucose) exert water shifts unlike urea (as well as ethanol)
Plasma Osmolality Is hyponatremia always associated with a low plasma osmolality? NO
Plasma Osmolality • Example • Serum Na+ = 125 mEq/L • BUN = 140 mg/dL • Blood glucose = 90 mg/dL • Calculated and measured osmolality = 305 mOsm/kg • Posm = 2 x 125 + 90/18 + 140/2.8 • In this case, hyponatremia is associated with an elevated plasma osmolality • Effective osmolality= 255 mOsm/kg (calculation excludes BUN) thus this patient may have symptoms of hypotonicity despite an elevated plasma osmolality
Plasma Osmolality Is plasma hypoosmolality always associated with hyponatremia? YES Posm ~ 2 x plasma [Na+]
Plasma Osmolality Is hyponatremia always associated with hypotonicity? NO
Plasma Osmolality • Example: • Serum Na+ = 133 mEq/L • BUN = 11 mg/dL • Blood glucose = 500 mg/dL • Effective osmolality (tonicity) = 294 mOsm/kg (2 x 133 + 500/18) • Hyponatremia is not always associated with hypotonicity and thus direct therapeutic intervention may not be required (in this example, treat underlying hyperglycemia)
Plasma Osmolality Do ineffective osmoles (urea, ethanol, ethylene glycol, methanol cause hyponatremia)? NO. Remember these osmoles readily move between fluid compartments without causing water shifts
Plasma Osmolality Do effective osmoles (glucose, mannitol) cause hyponatremia? Yes. These osmoles shift water out of the cells
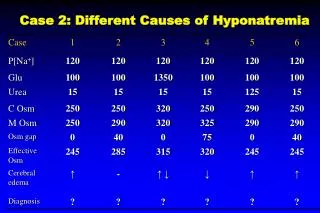
Clinical Examples of Hyponatremia • Plasma Na+ = 120 mEq/L • Blood glucose = 90 mg/dL • BUN = 14 mg/dL • Calc Posm = 250 mosmol/kg • Meas Posm = 250 mosmol/kg • Osmolar gap = 0 mosmol/kg • Tonicity = 245 mosmol/kg Hypotonic hyponatremia risk of cerebral edema
Clinical Examples of Hyponatremia • Plasma Na+ = 120 mEq/L • Blood glucose = 90 mg/dL • BUN = 14 mg/dL • Calc Posm = 250 mosmol/kg • Meas Posm = 290 mosmol/kg • Osmolar gap = 40 mosmol/kg • Tonicity = 285 mosmol/kg Pseudohyponatremia ( lipids, protein) Note: absence of osmolar gap rule out this diagnosis No risk of cerebral edema
Clinical Examples of Hyponatremia • Plasma Na+ = 120 mEq/L • Blood glucose = 1350 mg/dL • BUN = 14 mg/dL • Calc Posm = 320 mosmol/kg • Meas Posm = 320 mosmol/kg • Osmolar gap = 0 mosmol/kg • Tonicity = 315 mosmol/kg Hyponatremia caused by hyperglycemia No risk of cerebral edema
Clinical Examples of Hyponatremia • Plasma Na+ = 120 mEq/L • Blood glucose = 90 mg/dL • BUN = 14 mg/dL • Calc Posm = 250 mosmol/kg • Meas Posm = 325 mosmol/kg • Osmolar gap = 75 mosmol/kg • Tonicity = 320 mosmol/kg Hyponatremia caused by mannitol [Mannitol] = 75 mmol/L Osmolar gap (≠ hyperglycemia) No risk of cerebral edema
Clinical Examples of Hyponatremia • Plasma Na+ = 120 mEq/L • Blood glucose = 90 mg/dL • BUN = 14 mg/dL • Calc Posm = 250 mosmol/kg • Meas Posm = 300 mosmol/kg • Osmolar gap = 50 mosmol/kg • Tonicity = 245 mosmol/kg Hyponatremia due to ethanol [EtOH] = 50 mmol/L risk of cerebral edema
Clinical Examples of Hyponatremia • Plasma Na+ = 120 mEq/L • Blood glucose = 90 mg/dL • BUN = 126 mg/dL • Calc Posm = 290 mosmol/kg • Meas Posm = 290 mosmol/kg • Osmolar gap = 0 mosmol/kg • Tonicity = 245 mosmol/kg Hyponatremia caused by renal failure risk of cerebral edema Note: a normal measured plasma osmolality does not preclude an increased risk of cerebral edema
Causes of Hyponatremia Current Medical Diagnosis & Treatment, 2009
Hypotonic Hyponatremia • Hypovolemic • ↓ [Na+] = ↓↓TBNa/↓TBW • Euvolemic • ↓ [Na+] = ↔ TBNa/↑TBW • Hypervolemic • ↓ [Na+] = ↑TBNa/↑↑TBW
Laboratory Approach to Hyponatremia • Start with plasma osmolality to exclude pseudohyponatremia (normal Posm) and hypertonic hyponatremia (elevated Posm) • When hypotonicity is confirmed, then assess clinically patients’ volume status
Urine Osmolality • Determine whether H2O excretion is normal or impaired • Uosm < 100 mosmol/kg indicates that ADH is appropriately suppressed • Primary polydipsia • Reset osmostat (when Posm is below normal) • Low solute intake • Uosm > 100 mosmol/kg occurs in majority of hyponatremic patients and indicates impaired H2O excretion
Urine Sodium Concentration • Una < 20 mEq/L • Hypovolemia due to extra-renal losses • Edematous states in CHF, cirrhosis, nephrotic syndrome • Dilutional effect in primary polydipsia due to very high urine output • Una > 20 mEq/L • Hypovolemia due to renal losses • Renal failure • SIADH • Reset osmostat
Other Labs • Plasma uric acid concentration • Hypouricemia (< 4mg/dL) in SIADH • Mild hypervolemia decreases proximal Na+ reabsorption, leading to increased urinary uric acid excretion • Blood urea nitrogen • BUN may be < 5mg/dL in SIADH • Mild hypervolemia leads to urinary urea wasting
Case Illustration 1 • 62 year old woman was admitted to the hospital for abnormal liver-function tests. She had a history of acute myelogenous leukemia and had undergone transplantation of T-cell depleted allogeneic bone marrow 2 years earlier. Medications include tacrolimus, prednisone, MMF, ursodiol, atovaquone, acyclovir and clarithromycin. Exam: afebrile, BP 130/75, HR 80. Appeared euvolemic. Labs revealed serum sodium level 124 mmol/L. What labs do you want to order? NEJM 2003; 349:1465-9
Case Illustration 1 • Serum osmolality 294 mOsm/kg • Urine osmolality 434 mOsm/kg • Urine sodium 62 mmol/L • BUN 43 mg/dL • Serum creatinine 1.4 mg/dL • Serum glucose 85 mg/dL Calculated plasma osmolality 268 mOsm/kg
Case Illustration 1 • Total serum protein 5.1 gm/dL • Lipemia was not observed • Lipid profile (2 years prior) • Total cholesterol 181 mg/dL • Triglyceride 136 mg/dL What would you do next?
Case Illustration 1 • Current lipid profile • Total cholesterol 1836 mg/dL • High-density lipoprotein 68 mg/dL • Very low-density lipoprotein 42 mg/dL • Triglyceride 208 mg/dL • Calculated low-density lipoprotein 1726 mg/dL • Serum [Na+] was 145 mmol/L when measured on a blood-gas machine What’s the cause for the patient’s hyponatremia?
Severe hypercholesterolemia causing pseudohyponatremia • Lipoprotein X • Reflux of unesterified cholesterol and phospholipids into the circulation from cholestatic biliary ducts • These cholesterol particles are insoluble in plasma water and thus increase the solid fraction of plasma • Occurs in patients with severe cholestasis (chronic graft-versus-host disease, primary biliary cirrhosis) • Serum is NOT lipemic (≠ severe hypertriglyceridemia)
Pseudohyponatremia • Each liter of plasma contains • ~ 930 ml water • ~ 70 ml proteins and lipids • High lipids or proteins reduce plasma water; thus plasma [Na+], measured per liter of plasma, is artifactually low • Plasma osmolality is unaffected • Osmometer measures only the Na+ activity in the plasma water Measurement by an osmometer What is the normal physiologic sodium concentration? ~ 151 mEq/L plasma water
Pseudohyponatremia Serum [Na+] = 140 mEq/L Serum [Na+] = 130 mEq/L Solids 7% Solids 14% 1 liter plasma HYPERLIPIDEMIA 1 liter plasma Water 93% HYPERPROTEINEMIA Water 86% Na+ 130 mEq in 860 ml Na+ 140 mEq in 930 ml OSMOLALITY Measures solute per unit plasma water 140 mEq/930 ml = 151 mEq/liter = 130 mEq/860 ml
Measurements of Serum [Na+] • Flame emission spectrophotometer (FES) • Measures serum [Na+] • Ion-selective electrode (ISE) • Measures [Na+] in plasma water • Two methods: • Direct potentiometry (using undiluted serum sample) • Blood gas machine • Indirect potentiometry (using diluted serum sample) • Pseudohyponatremia can occur with FES or indirect potentiometry, but not direct potentiometry
Flame Emission Spectrophotometer • Ultrafine spray of diluted serum sample is blown across a flame • Measures the intensity of the light emitted at the wavelength characteristic of sodium • Intensity is directly proportional to the # sodium atoms in the sample • Sample is compared to a standard aqueous solution of known [Na+]
Ion-Selective Electrode • Measures electrical potential across a sodium-selective membrane immersed in the serum sample • Electrical potential is a function of the Na+ activity in the sample, which correlate with sodium concentration in serum water (in undiluted serum)
Case Illustration 2 • 43-year old woman with persistent renal failure two months after a liver transplant, developed acute hyponatremia during treatment of thrombocytopenia with intravenous immune globulin (in 10% maltose). Before therapy, her serum [Na+] was stable at 131 mmol/L. One gm/kg of IVIG was administered over 12 hours on 2 successive days. After the second infusion, her serum [Na+] was 118 mmol/L. After 4 hours of hemodialysis, the serum [Na+] was 133 mmol/L. Hyponatremia recurred during each of the four successive infusions of IVIG. Direct potentiometry was used for the sodium assay. What’s the cause for this patient’s hyponatremia?
Case Illustration 2 Annals of Internal Medicine 1993;118:526-8
Hypertonic Hyponatremia • Effective osmoles result in water movement out of cells, decreasing plasma [Na+] by dilution • Causes • Hyperglycemia-most common • Mannitol • Sorbitol • Glycerol • Radiocontrast agents
IVIG Causing Hyponatremia • Hypertonic hyponatremia due to maltose intoxication • Maltose given intravenously is normally metabolized by maltase in the renal proximal tubule and excreted in the urine • Metabolic products of maltose metabolism can accumulate in the setting of renal failure, raising the plasma osmolality and causing dilutionalhyponatremia • Pseudohyponatremia • IVIG increases the protein-containing nonaqueous phase of plasma* *NEJM 1998; 339:632
Case Illustration 3 • Late on the afternoon of 1 June 1981, a 46 year old woman was admitted in a coma to a hospital in Durban, South Africa. Before dawn that day, she had begun a 90 km marathon race. But 20 km from the finish line, she failed to recognize her husband who had come to assist her. He convinced her to stop running and drove her to the hospital. There she received two liters of IV fluid but then suffered a grand mal seizure and lapsed into coma. Serum [Na+] was 115 mmol/L. CXR showed evidence of pulmonary edema. First case report of exercise-associated hyponatremia complicated by encephalopathy and non-cardiogenic (neurogenic) pulmonary edema Br J Sports Med 2006;40:567-72
Case Illustration 3 What would be your immediate treatment for this patient’s hyponatrema? I would give her 100 ml of 3% saline over 10 minutes
Acute Symptomatic Hyponatremia (<48 hours): Treatment • Immediate goal: ↑ [Na+] by 1-2 mEq/L/hr using 3% NS ± Lasix • 3% NS infusion at 1-2 ml/kg/hour or • 100 ml of 3% NS over 10 minutes, raising serum [Na+] 2-3 mEq/L in a short period of time • If neurologic symptoms persist or worsen, can repeat 100 ml bolus 1 or 2 more times at 10-minute intervals • Aim for cessation of neurologic symptoms, then reduce correction rate • Goal increase in serum [Na+] • First 24 hours: < 8-10 mEq/L • First 48 hours: < 18 mEq/L
Why the urgency to treat? minutes hours days NEJM 2000; 342:1581-9
Symptoms of Hyponatremia • Signs and symptoms • < 125-130 mEq/L: nausea, vomiting (earliest findings) • < 115-120 mEq/L: headache, lethargy, obtundation • < 110-115 mEq/L: seizures, coma, respiratory arrest • Severity of neurologic dysfunction (cerebral edema) is related to the rapidity of decline and level of plasma Na+ concentration • Cerebral edema occurs primarily with rapid (over 1-3 days) reduction in plasma [Na+]
Exercise-Associated Hyponatremia Occurrence of hyponatremia (< 135 mEq/L) during or up to 24 hours after prolonged physical activity
Risk Factors for EAH • Excessive drinking (>1.5 L/hr) during event- major risk • Exercise duration > 4 hrs or slow exercise pace • Low body weight (overhydration in proportion to size) • Female gender (may be explained by lower body weight) • Pre-exercise overhydration • Abundant availability of drinking fluids at event • NSAIDS (not all studies) • Extreme hot or cold environment
EAH: Overhydration • Increased fluid intake associated with substantial weight gain during the activity increases risk of hyponatremia • Athletes who gained > 4% body weight during exercise had a 45% probability of developing hyponatremia • However, excessive fluid consumption is not the sole explanation for development of EAH • Hyponatremia did not develop in 70% of the athletes who overconsumed fluids and had an increase in body weight Proc Natl Acad Sci USA 2005; 102: 18550-5
Figure 1. Pathophysiologic factors in the development of exercise-associated hyponatremia (EAH) Rosner, M. H. et al. Clin J Am Soc Nephrol 2007;2:151-161
Therapy of EAH • Mild, asymptomatic hyponatremia (130-135 mEq/L) • Fluid restriction and observation until spontaneous diuresis occurs • Avoid IV 0.9% normal saline due to risk of worsening hyponatremia • Severe, symptomatic hyponatremia • Hypertonic saline (3% NS) • No cases of osmotic demyelination have been reported with treatment of EAH • Indicated in patients manifesting encephalopathy and non-cardiogenic pulmonary edema • Vaptans-no data to indicate efficacy
EAH: Neurogenic Pulmonary Edema Exercise-Associated Hyponatremia: Why Are Athletes Still Dying? Moritz, Michael; Ayus, Juan Clinical Journal of Sport Medicine. 18(5):379-381, September 2008. DOI: 10.1097/JSM.0b013e31818809ce Mechanism of non-cardiogenic pulmonary edema in exercise-associated hyponatremia.
EAH: Neurogenic Pulmonary Edema A depiction of the Ayus-Arieff syndrome. Hyponatremia produces cytotoxic cerebral edema which in turn leads to a neurogenic pulmonary edema. Pulmonary edema leads to hypoxia, which impairs brain cell volume regulation, resulting in a vicious cycle of worsening cerebral edema and pulmonary edema. This syndrome can be reversed by the prompt administration of 3% NaCl. Exercise-Associated Hyponatremia: Why Are Athletes Still Dying? Moritz, Michael; Ayus, Juan Clinical Journal of Sport Medicine. 18(5):379-381, September 2008. DOI: 10.1097/JSM.0b013e31818809ce
Prevention of EAH • Avoid over consumption of fluids before, during and after exercise • Drink only according to thirst and no more than 400-800 ml per hour • Monitor body weight to avoid weight gain • No evidence that sports drinks can prevent EAH • Most drinks have sodium content 10-20 mEq/L (hypotonic) • No evidence that sodium supplementation can prevent EAH
Case Illustration 4 • 70 year old woman was admitted for coronary angiography after developing chest pain. Mild HTN had been detected 8 months previously, followed by treatment with HCTZ. On admission, serum sodium was normal at 140 mEq/L. Weight 70 kg. After the catheterization, pt was encouraged to increase her fluid intake, and over the next 24 hours she drank 5 L of water. On HOD #3, serum sodium was 127 mEq/L. On the following day, she underwent an angioplasty and was once again advised to increase her fluid intake. The next morning the patient complained of fatigue, nausea, headache and dizziness; BP 95/60. Serum sodium was 118 mEq/L. SMJ 1986; 79: 1456-7