Download
1 / 26
280 likes | 534 Views
Hyponatremia. Debra Bynum,MD Division of Geriatric Medicine. Clinical Case.

E N D
Hyponatremia Debra Bynum,MDDivision of Geriatric Medicine
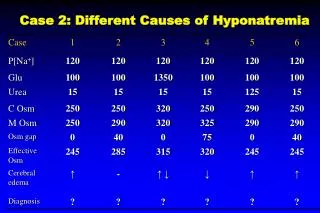
Clinical Case • An 82 y/o woman is admitted from a nursing home with confusion. She has had a poor appetite over the past year with significant weight loss. Two weeks ago HCTZ was added. Over the past few days, the nurses note some n/v, no diarrhea, fever or other complaints. • On exam, she has some dry oral mucosa but she is not orthostatic. There is no evidence of CHF, ascites or edema. She is awake, but lethargic. Neuro exam is nonfocal. Labs: Na 121 (last 130 4 weeks ago), normal renal/liver function. Serum osm 250, urine osm 280, urine Na 30.
Pretest • 1. What are the potential Causes of hyponatremia in this patient? • 2. Does her urine osm of under 300 rule out SIADH? • 3. What other laboratory data is needed? • 4. How might her diet be contributing to her hyponatremia? • 5. How is the urine Na helpful? What in this case would limit its usefulness? • 6. How does water intake or relatively hypotonic fluid intake worsen hyponatremia with SIADH?
The Forces Behind Na and water • Intracellular volume maintained by regulation of plasma osmolality (changes in water balance) sensed by hypothalamic osmoreceptors and affected by ADH and the thirst mechanism via changes in water intake and urine osmolality • Plasma volume ultimate goal; maintained by regulation of Na balance;sensed by afferent arteriole, carotid sinus, cardiac atria and effected by renin-angio-aldo system, sympathetic nervous system, ADH and atrial natriuretic peptide acting on urine na excretion
Euvolemic SIADH Relatively high urine osm (>100, often >300) High/normal urine Na (>40) hypouricemia/urinary urea wasting Hypothyroidism ADH Like compounds (prolactinoma, HCG, waldenstrom’s) Primary Polydipsia Low urine Osm (<100) Intake over 10 L/day Hypovolemic appropriate ADH urine na <20 (unless diuretic use) high urine osm (ADH) hyperuricemia/ dec urinary uric acid Hypervolemic CHF, cirrhosis, nephrotic syndrome “appropriate ADH” low urine Na high urine osm (ADH) poor prognostic factor Hyponatremia
ADH • “antidiuretic” • central role in most all causes of hyponatremia; must just determined whether ADH is appropriate, “semi appropriate”, or inappropriate • Stimulation of release: nausea/vomiting, pain, volume depletion
SIADH • Does not in itself cause edema (activation of volume receptors leads to release of urine na and water) • Symptoms relate to rapidity of change • 115-120: headache, lethargy, obtundation • 110-115: coma, seizures
SIADH • Causes: • CNS: neoplasms, bleed, guillain-barre, SIP, sarcoidosis (hypothalamic involvement), pituitary surgery, nausea • Drugs: SSRI, thiazide diuretics, carbamazepine, haloperidol, amitriptyline, bromocriptine… • Pneumonia, TB, ARDS, malignancy • Ectopic ADH: carcinomas (small cell), pancreatic or duodenal ca, thymic ca • ADH like compounds: prolactinoma, Waldenstrom’s
Increased ADH> renal water retention> increased body water Body fluid dilution hyponatremia dec urine osm over time with new steady state for water hyponatremia persists until water restricted and excess water dissipated Water intake> renal water retention > increased body water increased ECF volume increased output, renal blood flow and decreased tubular reabsorption of na (maintain normal volume!) increase na excretion (stretch receptors – inc natriuretic peptides…) hyponatremia new steady state for na SIADH: Persistent Hyponatremia
SIADH: Treatment • Water restriction • Aggressive treatment (3% saline, +/- furosemide) not indicated unless symptomatic, acute, or na <110 • no faster than .5 meq/L per hour correction (to avoid risk of central pontine myelinolysis) • once na reaches 120, water restriction only
Volume Depletion • True volume depletion due to vomiting, diarrhea, bleeding, urinary losses • n/v also stimulate ADH release (to maintain circulating volume) • Adrenal Insufficiency (lack of cortisol resulting in decreased na reabsorption plus volume depletion)
Volume Depletion: Treatment • Carefully monitor sodium as fluids given to prevent overly rapid correction • goal .5 meq/L per hour correction • Degree that 1 L fluid will raise plasma Na conc: Increase PNa= (infusate [Na] -Pna) / (TBW +1) • Isotonic saline: • raises plasma sodium by 1-2 meq/L for every liter of fluid infused since saline has higher Na concentration (154 meq/L) than hyponatremic plasma • volume repletion removes stimulation of ADH
Thiazide Diuretics • Elderly women at higher risk • Element of volume depletion • Not seen as often with loop diuretics (inhibition of NaCl transport in loop of Henle prevents generation of countercurrent gradient and limits ability of ADH to induce water retention) • May result in normal/increased urine Na, even though underlying volume depletion;
CHF, Cirrhosis, Nephrotic syndrome • CHF/Cirrhosis: pressure sensed at carotid sinus baroreceptors reduced due to poor cardiac output or peripheral vasodilation/poor circulating volume; associated with higher mortality; degree of hyponatremia as prognostic marker • Nephrotic syndrome: usually due to renal disease rather than poor circulating volume
Primary Polydipsia • Psychiatric disorder, often complicated by increased thirst with antipsychotic meds • can occur with hypothalemic lesions (sarcoid or other infiltrative processes) • Usually no hyponatremia unless intake over 10-15 L/day, or acute 3-4 L water load • Urine osm below 100 (NOT ADH problem!) • Increased problems if other ADH stimulus (n/v, anxiety)
Low Dietary Solute Intake • “Tea and Toast” Diet • Beer drinkers: Beer Potomania • Normally excrete 600-900 mosmol/kg solute daily (if minimum urine osm is 60 mosmol/kg, max urine output will be 10-15L/day: 900mosm/day / 60 mosmol/kg = 15) • If daily intake poor, daily solute excretion may fall below 250 mosmol/kg, reducing the maximum urine output to below 4 L day; Hyponatremia develops if greater than 4 L consumed in day • Urine appears dilute (osm of 100)
Pseudohyponatremia • Plasma osmolality that is normal or elevated • usually not at risk for hypoosmolality induced cerebral edema • Lipids, proteins • Not a problem with labs that directly measure na
High plasma osmolality • Hyperglycemia • mannitol • IVIG with maltose retention in patients with renal failure • Glycine: TURP; exception to rule that patients with hyperosm hyponatremia do not get into trouble; complicated by urinary retention, n/v, postsurgical state; severe hyponatremia after urological procedure should be treated acutely with saline/furosemide!
Back to the Case... • 1. What are the potential causes of hyponatremia in this patient? • Thiazide diuretic (complicating urine na) • underlying SIADH (suggested by inappropriately high urine osm) • recent n/v and volume loss (although not orthostatic) • poor solute intake/ “tea and toast” diet ( may be reason that urine osm is not as high as would be expected with SIADH alone) • ?CNS event (stroke, subdural)
Case... • 2. Does her urine osm of under 300 rule out SIADH? • No; classically urine osmolality is 300 or greater, but the urine osm of 220 in the setting of a serum na of 121 is inappropriately elevated (over 100 really is inappropriate)
Case... • 3. What other laboratory data would be needed? • TSH • Cortisol level (although not orthostatic) • probably neuroimaging given underlying dementia and risk for CVA, subdural, etc • consider uric acid to help differentiate hypovolemia from SIADH (hypouricemia in SIADH, elevated/normal uric acid if dehydrated)
Case... • 4. How might her diet be contributing to her hyponatremia? • Poor solute intake could result in dilute urine and hyponatremia as discussed previously
Case... • 5. How is the urine Na helpful in differentiating SIADH from hypovolemia? What in this case would limit its usefulness? • Urine Na should be normal/elevated with SIADH and should be low with hypovolemia • thiazide diuretic use may elevated urine na temporarily
Case... • 6. How does water intake or hypotonic fluid intake worsen the hyponatremia with SIADH? • Example: patient with SIADH, urine osmolality of 616 mosmol/kg; 1 liter of NS has 308 mosmol of NaCl, 1000 cc H2O; • Isotonic Saline NaCl H2O • In 308 1000 ml • Out 308 500 ml (conc 616) • Net 0 +500 of free H2O!
Case... • 7. How would you manage this patient? • Water restriction? Need to address amount of intake she has had • Avoid rapid correction (osmotic demylination) • Discontinuation of Thiazide • Would probably not give IVF initially as most may be due to thiazide, SIADH, poor diet, although may be complicating element of hypovolemia; if n/v persisted after holding thiazide, consider small amount of normal saline (relatively hypertonic with urine osm of 220)