Download
1 / 57
1.07k likes | 2.51k Views
Hyponatremia Management. Ganesh Shidham, MD Division of Nephrology. Outline ……. Role of ADH in Hyponatremia Incidence and Mortality Mechanism of Hyponatremia Identifying types of Hyponatremia Clinical features and Brain Adaption Treatment Complications of treatment. Hyponatremia.

E N D
Hyponatremia Management Ganesh Shidham, MD Division of Nephrology
Outline …… Role of ADH in Hyponatremia Incidence and Mortality Mechanism of Hyponatremia Identifying types of Hyponatremia Clinical features and Brain Adaption Treatment Complications of treatment
Hyponatremia Sodium Water “Hyper-acquemia”
Normal water balance Normal water intake 1-1.5 L/d Water Of Cellular Metabol 0.3-0.5 L/d Water intake Intracellular Extracellular Compartment compartment 28 L 14 L 42 L TBW 60% of body weight ADH Variable water excretion Kidney Fixed water excretion Stool Sweat Lungs 0.1 L/d 0.1 L/d 0.3 L/d Water excretion Total insensible losses 0.5 L/d Total urine output 1-1.5 L/d
Neurohypophysis • Consists of: • Supraoptic Nucleus • Para ventricular nucleus • Axons of Pituitary stalk • Neuron terminals in • posterior pituitary
ADH stimuli: 1-3% ↑ osmolality 10-15% ↓ vol /BP Other stimuli: Pain Nausea Stress Medications
Maximal ADH No ADH Changes in urinary volume and Osmolality along the Nephron
Lumen V2 receptor AQP 2 – Aquaporins ADH action on distal nephron
Incidence And Mortality
Prevalence of Dysnatremia 303,577 samples from 120,137 patients 28.2 Acute Hospital care 21 Ambulatory hospital care Community care Prevalence % 7.2 1.43 0.53 0.72 0.06 0.01 0.01 0.49 0.17 0.03 Na < 116 Na < 135 Na > 145 Na > 165 Hawkins. Clin Chim Acta 337:169-172, 2003
Hyponatremia Mortality (due to change in Brain volume)
Mechanism of Hyponatremia
Hyponatremia Supervenes when free water intake >> free water excretion Main defense excretion of free water by kidneys
Hypotonic Hyponatremia caused by: Dilution from retained water OR Depletion of electrolytes in excess of water
Identifying types of Hyponatremia
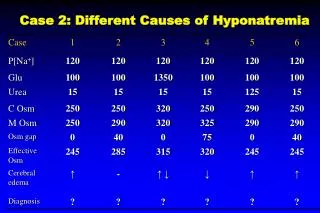
Hyponatremia Serum Osmolality Normal Low High (280 - 295 mOsm /kg) (<280 mOsm /kg) (>295 mOsm /kg) Isotonic Hypotonic Hypertonic Hyponatremia (Pseudohyponatremia) Hyponatremia Hyponatremia (Translocational) 1.Hyperglycemia 2.Mannitol, Sorbitol Glycine 3.Radiocontrast agent 1.Hyperproteinemia 2.Hyperlipidemia Volume status
Hypotonic Hyponatremia Hypovolemic Euvolemic Hypervolemic Urine Na 1.SIADH 2.Glucocorticoid def 3.Hypothyroidism 4.Poor solute intake -Tea Toast syndrome - Beer potomania 5.Post op / Hospital acquired 1.CHF 2.Cirrhosis 3.Nephrotic synd 4.Advanced CRF <30 >30 ExtraRenal Renal 1.Diarrhea 2.Vomiting 3.Hemorrhage 4.Sweating 1.Diuretics 2.Mineralocorticoid def 3.Salt loosing Nephropathies 4.Cerebral salt wasting
Hypertonic HyponatremiaEffect of Glucose on Serum Na Correction factor: Increase Na by 1.6 to 2.4 per 100 glucose
Hypotonic hyponatremia (Vol status indeterminate) Urine Na <30 : Respond to 0.9 NS Volume depleted Urine Na > 30 : No response to 0.9 NS Likely to have SIADH
Euvolemic Hypotonic Hyponatremia SIADH Criteria for diagnosis: 1. P osm <275 mOsm/kg 2. U osm >100 mOsm/kg 3. Clinical euvolemia 4. Urine Na > 30mmol/L while on normal salt intake 5. Normal thyroid, adrenal and renal functions 6. Inappropriately elevated AVP levels in 85-90%
Euvolemic Hypotonic Hyponatremia SIADH : Common Causes
Euvolemic Hypotonic HyponatremiaSIADH : Treatment • Discontinue offending agent • Treatment of etiology (infection, pain) • Fluid restriction (for Chronic asymptomatic Hyponatremia)
Urinary solute excretion in person on normal diet- 800-900 mM/day Urinary solute excretion Urinary Osmolality Euvolemic Hypotonic hyponatremiaPoor solute IntakeBeer Potomania, Tea Toast syndrome Urine Volume = Clinical setting of low solute intake: - Alcoholism (Beer Potomania) - Anorexia (Tea and Toast Diet)
Euvolemic Hypotonic hyponatremiaPoor solute IntakeBeer Potomania, Tea Toast syndrome • Normal Solute excretion = 900 mOsm/d • Assume maximal urine dilution= 60 mOsm/kg Urine Volume = 900/60 = 15 L/d • With solute excretion of 300 mOsm Urine Volume = 300/60 = 5 L/d • With solute excretion of 300 mOsm and maximal urine dilution of 150 mOsm/kg Urine volume = 300/150 = 2 L/d
Euvolemic Hypotonic hyponatremiaPoor solute IntakeBeer Potomania • Assume Beer consumption of 5 L: Na intake 10 mM K intake 50 mM Obligatory urea excretion 90 mM Total solutes 150 mOsm • Assume urine dilution of 50 mOsm/kg • Urine volume = 150/50 = 3 L • 2 L of fluids (hypotonic) is retained to produce hyponatremia Beer: Na 2 mM/L K 10 mM/L
Euvolemic Hypotonic hyponatremiaPoor solute IntakeTreatment • Increase solute intake – • High protein diet • Salt tablets or high dietary salt • Urea 2. Fluid restriction
Hospital acquired Hyponatremia • Virtually every hospitalized patient has potential stimulus for AVP excess • Administration of hypotonic fluid with excess AVP are at risk for Hyponatremia Chung HM et al, Arch Inter Med 2002
Hospital acquired hyponatremia • Series of 15 women with Hyponatremia and permanent neurological damage • Following elective surgery • 11 had received 5% Dextrose post surgery Arieff AI et al, NEJM 1986
Hospital acquired hyponatremia • Series of 65 patients with Hyponatremia and encephalopathy • Following elective surgery • All had received hypotonic fluid Ayus JC et al, Ann Intern Med, 1992
Hospital acquired hyponatremia • Odds ratio for developing hyponatremia was 3.7 for each liter of electrolyte-free water given to 70 kg patient Aronson D et al, Am J Kid Dis. 2002
Hospital acquired hyponatremia • Ringer’s Lactate (Sodium 77) is hypotonic and can produce hyponatremia • No justification for Ringers lactate in post op period • Administration of 0.9 saline is safe • No reports of 0.9 Saline causing neurological complications of hyponatremia Steele A et al, Ann Intern Med 1997 Moritz ML et al, J Am Soc Nephrol 2005
Clinical features And Brain Adaption
Hyponatremia Symptoms
Cerebral adaption to decrease cerebral edema • Early 1-3 hrs • CSF distribution • Later (> 3 hrs) • Loss ofOsmolytes and electrolytes: • Glutamate, Inositol, Taurine, • Urea, K, Na, Creatinine
Acute Hyponatremia: • Less than 48 hrs • Neurologic symptoms due to brain edema • Rapid correction well tolerated • Chronic Hyponatremia: • More than 48 hrs or unknown time • Mild brain edema (<10%) • Sensitive to Na correction rate • Aim to increase Na by 10% (not more than 12 in 24 hrs)
Treatment of Hyponatremia: Balance – Risk of Hyponatremia Vs Risk of Correction
Treatment of Hyponatremia • How long has hyponatremia been present? • Does the patient have symptoms? • Does the patient have risk factors for development of neurologic complications?
Monitoring of patients: • Volume status • Daily weight • Frequent Serum Na, K • Plasma Osmolality • Urine Na, K, osmolality • Strict Input and Output
Treatment of HyponatremiaBasic concept • Free water intake << Free water output AND Na, K intake >> Na, K output 2. Needed Info: • Serum Na , osmolality • Urine Na, K, Osmolality • Strict Input/ Output 3. Rate of correction
TreatmentSymptomatic Hyponatremia • Treatment based on neurological symptoms and not on Sodium • Needs aggressive management with 3%NaCl • No role of fluid restriction alone • Treatment should precede any neuroimaging • Treatment in monitored setting • Sodium levels measured every 2 hours
TreatmentSymptomatic Hyponatremia • Impending herniation: Sz, resp arrest,, obtundation, Decorticate posturing, dilated pupils: - 100 ml of 3% NaCl as a bolus over 10 min to rapidly reverse brain edema. - Repeat bolus as required till symptoms improve • Encephalopathy: Headache, N/V, Altered mental status: - 3% NaCl @ 50-100 ml/hr • Calculating 3% saline rate: Weight in kg x desired rate of increase in Serum Na
TreatmentSymptomatic Hyponatremia 4. Monitor [Na] every 2-4 hrs 5. Stop active correction when appropriate end point is reached: - Patient becomes asymptomatic - Safe Na levels reached (generally 120) - Total correction 12 mmol in 24 hrs or 18-20 mmol in 48 hrs 6. Complete rest of correction with - fluid restriction
Treatment Asymptomatic Hyponatremia • Attend to underlying cause • No immediate correction needed • Fluid restriction D Ellison, T Berl. NEJM 2007;356:2064-72