Download
1 / 57
570 likes | 582 Views
Family Retroviridae. Genus Lentivirus. Human Immunodeficiency Virus.

E N D
Family Retroviridae. Genus Lentivirus. Human Immunodeficiency Virus
2008, Françoise Barré-Sinoussi and Luc A. Montagnier were awarded Nobel prizemedicine for their role in the discovery of “the virus that causes AIDS”. More than two decades ago (1983) they identified a virus they named LAV(lymphadenopathy virus), which later became known as HIV. Barré-Sinoussi Luc A. Montagnier
HIV and AIDS: a Global Pandemic • First cases identified June, 1981 • World estimates (as of 2011): • > 34 million living with HIV • 30 million deaths since 1981 • 7 000 people become infected and 6 000 people die of AIDS daily. • During 2011: 2,5 millionbecame infected and 1,7 million people died. • In Ukraine (as of 2011): • 214 000 HIV-infected persons • 28 000 deaths since 1987
Global view of HIV infection • The overwhelming majority of people with HIV live in the developing world. • Sub-Saharan Africa accounts for two-thirds of all infected people (67 %). • South and South-East Asia has the second highest number of infected people.
Adults and children estimated to be living with HIV, 2011 Eastern Europe & Central Asia 1.4 million [1.3 – 1.5 million] Western & Central Europe 820 000 [720 000 – 910 000] North America 1.5 million [1.2 – 2.0 million] East Asia 770 000 [500 000 – 1.0 million] Middle East&North Africa 460 000 [400 000 – 530 000] Caribbean 240 000 [220 000 – 270 000] South & South-East Asia 4.1 million [3.7 – 4.6 million] Sub-Saharan Africa 22.5 million [20.9 – 24.2 million] Latin America 1.4 million [1.2 – 1.6 million] Oceania 57 000 [50 000 – 64 000] Total: 34 million
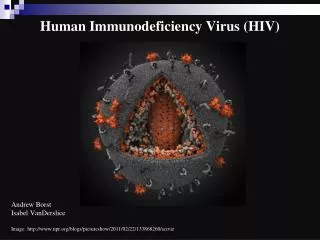
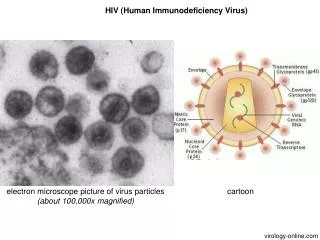
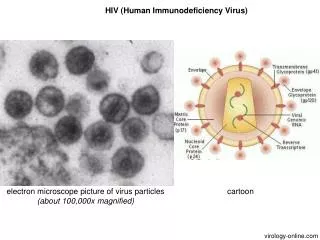
Electron microscopy of HIV • HIV is a spherical enveloped virus, about 90-120 nm in size. • The nucleocapsid has an outer icosahedral shell and inner coneshaped core, enclosing the ribonucleoproteins.
Attachment of HIV to a CD4+ cell • The glycoprotein gp 120 binds to the CD4 protein on T-helper cells and macrophages. • The glycoprotein gp 41 allows fusion of the virus with the cell membrane. Target cells: CD4 cells: Т-helpers Monocytes Macrophages Other cells: natural killers dendritic cells В-lymphocytes of the memory neuroglia astrocytes colonic epithelium endothelium
Chemokine receptors CCR5 or CXCR4 are co-receptors for HIV to enter target cells • CCR5 is expressed on T cells, macrophages, and microglia, CXCR4 on T cells. • They play a role in inflammatory responses to infection. The natural chemokines bind to this receptors and activate chemotaxis of immune cells. • When the CD8+ cells effectively make a large quantity of the chemokines, they may block the CCR5 and suppress HIV infection. • Conversely, when levels of the chemokines are low or absent, the virus is free to more easily infect cells. • A number of new HIV drugs, called entry inhibitors, have been designed to interfere with the interaction between CCR5 and HIV.
Resistance to HIV • CCR5-Δ32 is a genetic variant of CCR5. • CCR5-Δ32 is a deletion mutation of a gene when a portion of it is missing, and it thus cannot produce a functional CCR5 receptor. • CCR5-Δ32 decreases the number of CCR5 proteins on the outside of the CD4 cell, which can have a large effect on the HIV disease progression rates. It is possible that a person with the CCR5-Δ32 receptor allele will not be infected with HIV R5 strains. • When people inherited a defective version of CCR5 from both parents, they appeared to be resistant to infection with HIV. • People with the partial CCR5 defect may progress to HIV disease more slowly than someone without the CCR5 defect.
Process of infection of HIV • Infection is transmitted when the virus enters the blood or tissues of a person and come into contact with a suitable host cell. - HIV can cross the epithelial barrier through a process known as transcytosis by M cell. - HIV is picked up by Ag-presenting cells, primarily dendritic cells. - T helpers are infected by HIV in mucosal associated lymphoid tissue. - HIV establishes a fulminant local infection within a few days, and then spreads quickly throughout the body. HIV binding via cell surface receptors
Potential mechanisms underlying cell-associated HIV transmission. • (a) Columnar epithelium • (b) Stratified squamous epithelium
HIV entry via immune cells within the vaginal mucosa and spread to systemic lymphoid organs
HIV half-lives • Activated cells that become infected with HIV produce virus immediately and die within 1 to 2 days. • The time required to complete a single HIV life-cycle is approximately 1.5 days. • Production of virus by short-lived, activated cells accounts for the vast majority of virus present in the plasma. • Resting cells that become infected produce virus only after immune stimulation; these cells have a half-life of at least 5-6 months. • Some cells are infected with defective virus that cannot complete the virus life-cycle. Such cells are very long lived, and have an estimated half-life of approximately 3 to 6 months.
Pathogenesis of AIDS • The primary pathogenic mechanism in HIV infection is the damage the CD4 T-lymphocytes. • The T4 cells decrease in number • T4:T8 (helper:supressor) cell ratio is reversed. • Ways that HIV can damage T4 cells by: • budding virus particles, • cyncytium formation, • cytotoxic T-cell-mediated lysis.
The interaction of a dendritic cell with a lymphocyte.HIV bound to the surface of the dendritic cell is clustered at the site of interaction between the two cells (arrow) Multinucleated cell (syncytium) in touch preparation from cut surface of enlarged lymph node from patient with HIV-1 infection
Pathogenesis • Infected T4 cells do not release normal amounts of interleukin-2, gamma interferon and other lymphokines. • Polyclonal activation of B-lymphocytes leads to hypergammalobulinemia. AIDS patients are unable to respond to new antigens. • Monocyte-macrophage function is also affected. As a result, chemotaxis, antigen presentation and intracellular killing by these cells are diminished. • Monocyte-macrophages escape immune surveillance and transport the infection to other organ systems, particularly the lungs and brain.
Transmission of HIV HIV is transmitted by: • blood, • breast milk, • semen, • vaginal secretions. – Saliva, urine, tears have very low titer HIV. – Minor mucosal trauma and certain STDs (HSV for example) facilitate transmission.
Routes of Transmission of HIV • Sexual Contact • Blood Contact - Needle sharing behavior: Injection drug use and other needle sharing - Blood and blood products transfusion • Tissue and organs donation: - Semen, cornea, bone marrow, kidney etc. • Perinatal: - Intrauterine; - During labor and delivery; - Breast feeding.
Shift in HIV transmission patterns in the US based on estimates from the CDC
Distribution and number of documented cases of occupational transmission of HIV among health care workers by occupation
Spectrum of HIV Infection • 1. Acute retroviral syndrome: within 2-4 weeks of acquiring HIV • 2. Asymptomatic or latent HIV infection: variable duration • 3. Persistent generalized lymphadenopathy (PGL) • 4. AIDS related complex (ARC): CD4 count<500 • 5. Advanced HIV infection or AIDS: CD4 count<200
HIV Pathogenesis • In the immediate period following exposure, HIV is present at a high level in the blood. • It then settles down to a certain low level (set-point) during the asymptomatic period. • There is a massive turnover of CD4 cells, whereby CD4 cells killed by HIV are replaced efficiently. • AIDS develops, when killed CD4 cells can no longer be replaced. • The profound immunosuppression seen in AIDS is due to the depletion of T4 helpers.
Acute/Early Infection Approximately 50% of individuals develop a flu-like or mononucleosis illness • symptoms: • fever, • headache, • rash, • myalgia, arthralgia, • gartrointestinal symptoms: diarrhea, nausea or vomiting, • neurologic symptoms: aseptic meningitis,encephalitis • lymphadenopathy, organomegaly. • Associated with very high viral load. • p24 antigen can be demonstrated at the beginning of this stage. • HIV antibody may be negative.
Asymptomatic HIV Infection • Variable duration of time (as little as 1 to 2 years to more than 15 years). • Steady state viral load Persistent generalized lymphadenopathy • Gradual fall in CD4 cell count • Enlarged lymph nodes, at least 1 cm, in diameter, in two or more noncontagious extrainguinal sites, that persist for at least three months AIDS related complex • Generalised lymphadenopathy and splenomegaly • Fever, malaise, night sweats, persistent diarrhea and marked weigh loss of more than 10 per cent of body weight • Herpes zoster, hairy cell leukoplakia, vaginal candidiasis, tuberculosis, salmonellosis • Increasing viral load • Decreasing CD4 cell count
HIV and T cells go to “war” • Continuous and highly productive replication of HIV occurs in all infected individuals, although the rates of virus production vary by up to 70-fold in different individuals • Average T 1/2 of an HIV infected cell in vivo is 2.1 days • About 10 billion HIV particles are produced daily • About 2.6 billion CD4+ T-cells are produced daily
HIV ultimately reduces T-helpers • As T-helper is central to many aspects of immune function there is decreased or altered function of ALL arms of the immune system. • Clinical manifestations are due not primarily to viral cytopathology but are secondary to the failure of immune responses. This renders the patient susceptible to opportunistic infections and malignancies. • An exception is the dementia and other degenerative neurological lesions seen in AIDS. These may be due to the direct effect of HIV on the CNS.
HIV-associated infections Bacteria:Fungi: Salmonella spp. Candida albicans Mycobacterium avium Crypticoccus neoformans complex Histoplasma capsulatum Mycobacterium Coccidioides immitis tuberculosis Pneumocystis carinii Protozoa:Viruses: Toxoplasma gondii Herpes simplex Isospora belli Cytomegalovirus Criptosporidium hominis
Pneumocystis carinii pneumonia P. carinii is the most frequent opportunistic infection seen with AIDS. It produces a pulmonary infection, called P.carinii pneumonia (PCP), but rarely disseminates outside of lung. The most common clinical findings are acute onset of fever, non-productive cough, and dyspnea. Diagnosis is made histologically by finding the organisms in cytologic (bronchoalveolar lavage) or biopsy material from lung, typically via bronchoscopy. With Giemsa stain the dot-like intracystic bodies are seen. The cysts of P. carinii stain brown to black with the Gomori methenamine silver stain.
Cytomegalovirus (CMV) Retinitis -Progressive, painlessvision loss. -There are extensive areas of hemorrhage, with white retinal exudates. - CMV may also cause fever, pneumonia, GI bleed, neutropenia.
Oral Hairy Leukoplakia is a white patch on the side of the tongue with a corrugated or hairy appearance.Causative agent: Epstein Barr virus Symptoms The presence of white or gray colored patches on tongue, gums, roof of mouth, or the inside of the cheeks of mouth. The patch may have developed slowly over weeks to months and be thick, slightly raised, and may eventually take on a hardened and rough texture. It usually is painless, but may be sensitive to touch, heat, spicy foods, or other irritation.
Candidaalbicans can produce invasive infections in esophagus, upper respiratory tract, and lung Herpes simplex virus infection involves the gastrointestinal tract, mainly the esophagus and the perianal region. Herpes zoster infection of the skin occurs prior to the onset of clinical AIDS Candidiasis Herpes zoster
Kaposi’s Sarcoma Kaposi's sarcoma (KS) produces reddish purple patches, plaques, or nodules over the skin and can be diagnosed with skin biopsy. Visceral organ (lung, gastrointestinal tract, liver) involvement eventually occurs in 3/4 of patients with KS.
Severe wasting in a patient with human immunodeficiency infection Dementia. HIV may cause direct cytopathogenic damage in the CNS. It can cross the blood-brain barrier and cause encephalopathy leading to loss of higher functions, progressing to dementia.
Laboratory diagnosis • 1. Antigen detection: ELISA (core antigen p24).In the fist few weeks after infection and in the terminal phase, the test is uniformly positive. • 2. Virus isolation:from the peripheral lymphocytes by co-cultivation of the patient’s lymphocytes with uninfected lymphocytes in the presence of interleukin-2. It is not suitable as a routine diagnostic test. • 3. Polymerase chain reaction. The gold standard for diagnosis in all stages of HIV infection. It becomes necessary particularly in the course of treatment. • 4. Antibody detection:IgM antibodies appear in about 4-6 weeks to months after infection, to be followed by IgG antibodies. • Screening tests: ELISA assay. • Confirmatory test: Western blot.
ELISA for HIV antibody Microplate ELISA for HIV antibody: coloured wells indicate reactivity
Strips of blot • Strip А – Positive control • Strip В – Light positive control • Strip С – Negative control • Strip D – Positive specimen (antibodies against HIV-1 are detected)
Therapy of HIV Infection • Nucleoside-Analog Reverse Transcriptase Inhibitors (NRTI) inhibit viral polymerase by incorporating into viral DNA (they are chain-terminating drugs). - Zidovudine (ZDV, Retrovir) first approved in 1987 - Stavudine - Lamivudine etc. • Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs) inhibit HIV replication directly by binding non-competitively to reverse transcriptase (first approved in 1997). - Nevirapine - Delavirdine • Protease Inhibitors are specific for the HIV-1 protease and competitively inhibit the enzyme, preventing the maturation of virions capable of infecting other cells. - Saquinavir (Invirase) first approved in 1995 - Ritonavir - Indinavir etc. • Fusion or Entry Inhibitors bind gp41 andprevent HIV from binding to or entering human immune cells (first approved in 2003). - Enfuvirtide (Fuzeon) • Integrase Inhibitors interfere with the integrase enzyme, which HIV needs to insert its genetic material into human cells (first approved in 2007). - Raltegravir (Isentress) • Chemokine receptor antagonists binds the CCR5 coreceptorand inhibit fusion of the cellular membranes (first approved in 2007). - Maraviroc.