Download
1 / 39
390 likes | 562 Views
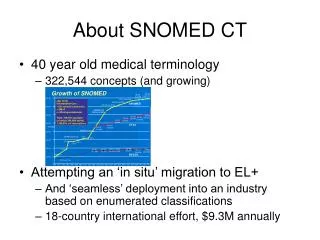
CDC-NPCR Pilot Projects Using SNOMED CT Encoded CAP Cancer Checklists. APIII Annual Conference Vancouver, British Columbia Ken Gerlach, MPH, CTR August 18, 2006. Role of Federal Government in Health Data Standards. The needed intervention is not for the government to set the standards, but

E N D
CDC-NPCR Pilot Projects Using SNOMED CT Encoded CAP Cancer Checklists APIII Annual Conference Vancouver, British Columbia Ken Gerlach, MPH, CTR August 18, 2006
Role of Federal Government inHealth Data Standards The needed intervention is not for the government to set the standards, but rather for them to convene the key players and to mediate. Donald W. Simborg J Am Med Informatics Assoc 1996;3(4):250
KY LA CA Federally Funded Cancer Registries, 2006 Seattle/ Puget Sound Detroit CT IA San Francisco/ Oakland NJ UT San Jose/ Monterey Los Angeles NM Atlanta ALASKA HAWAII * ` † NPCR REPUBLIC OF PALAU PUERTO RICO SEER *National Program of Cancer Registries (CDC) †Surveillance, Epidemiology, and End Results Program (NCI) VIRGIN ISLANDS NPCR/SEER
United States Cancer Statistics: 2003 Incidence and Mortality • Covers 96% of US population for incidence, 100% for mortality • State, regional, and national data • Rates for whites, blacks, Asians/Pacific Islanders, Native Americans, and Hispanics • http://www.cdc.gov/cancer/npcr/uscs
VIRGIN ISLANDS Geographic Coverage of USCS, 2003 Seattle/Puget Sound WA ME MT ND MN OR VT NH WI ID MI SD NY MA WY Detroit CT RI PN IA San Francisco/Oakland NE NJ NV OH IN IL UT DE MD San Jose/ Monterey CO WV VA DC KS MO CA KY Los Angeles NC TN OK AZ SC AR NM Atlanta MS AL GA LA TX AK REPUBLIC of Palau FL HAWAII Registry contributed incidence data; all states contributed mortality data PUERTO RICO
Importance of Pathology Data for Cancer Surveillance • > 92% cancer histologically-confirmed in pathology laboratories • Histology and Cytology • Key for complete and timely data • Rapid Case-Ascertainment • For cancers of special interest • Case-control studies • Clinical Trials
Hospital B HL7 File: Cancer Abstract HL7 File: De-identified Cancer Abstract HL7 File: Clinical HOSPITAL REGISTRY CENTRAL REGISTRY NATIONAL PROGRAMS Summarize Consolidate HL7 File: Patient Demographics Hospital C Private Physician Reference Path Lab Proposed Cancer Registry Data Flow Hospital A
North American Association of Central Cancer Registries (NAACCR) • Umbrella organization • Population-based cancer registries • Governmental agencies • Professional associations • Private groups • Purpose: To improve quality and use of cancer data www.naaccr.org
Cancer Protocols Project Workflow Laboratory System Hospital Cancer Registry Central Cancer Registry Receive Specimen from Surgeon Receive Report ______________________ Exit/Send acknowledgement Receive Report ______________________ Exit/Send acknowledgement Prepare and Analyze Specimen Cancer? Yes Input Data into CAP Checklist Format Checklist: PHIN Standards Transmit Checklist To physician
A CDC-led effort to improve public health communications by using and promoting health data and technology standards that electronically enable: - detection and monitoring - data analysis - knowledge management - alerting - response
Reporting Pathology Protocols (RPP) • Demonstration projects funded by CDC NPCR • Implement SNOMED CT Encoded CAP Cancer Checklists • In 2001 • California and Ohio • Cancers of the colon and rectum • In 2004 • California, Maine, and Pennsylvania • Cancers of the breast, prostate, and melanoma of the skin
RPP2 Laboratory Participants • Funded in 2004 • California • City of Hope Hospital National Medical Center, California • Maine • Maine Medical Center and • Dahl Chase Labs • Pennsylvania • University of Pittsburg Medical Center
CoC Cancer Program - Standard 4.6 • The CoC requires that 90 percent of pathology reports that include a cancer diagnosis will contain the scientifically validated data elements outlined on the surgical case summary checklist of the College of American Pathologists (CAP) publication, Reporting on Cancer Specimens. • Protocols not Checklists
RPP1 Project - Process • Identify question concepts on Checklist without a LOINC code • Presentation to LOINC for codes • Clarify Content and Suggest Revisions to the Checklist with CAP Cancer Committee • Development and Consensus on Implementation Tables • Development of Evaluation Measures
RPP1 Vocabulary • Logical Observations and Identifiers Names and Codes (LOINC) • Question – Metadata - Header - Data Item Name • Systematic Nomenclature of Medicine, Clinical Terms (SNOMED CT) • Answer – Data - Checkable line item - Data Item Codes
RPP2 Vocabulary • Systematic Nomenclature of Medicine, Clinical Terms (SNOMED CT) • Question – Metadata - Header - Data Item Name • Systematic Nomenclature of Medicine, Clinical Terms (SNOMED CT) • Answer – Data - Checkable line item - Data Item Codes
SNOMED CT Encoded CAP Checklist TUMOR SITE [R-0025A, 371480007] Tumor site (observable entity) ___ Cecum [T-59100, 32713005] Cecum structure (body structure) ___ Right (ascending) colon [T-59400, 51342009] Right colon structure (body structure) ___ Hepatic flexure [T-59438, 48338005] Structure of right colic flexure (body structure) ___ Transverse colon [T-59440, 485005] Transverse colon structure (body structure) ___ Splenic flexure [T-59442, 72592005] Structure of left colic flexure (body structure) ___ Left (descending) colon [T-59450, 55572008] Left colon structure (body structure) ___ Sigmoid colon [T-59470, 60184004] Sigmoid colon structure (body structure) ___ Rectum [T-59600, 34402009] Rectum structure (body structure) ___ Not specified [T-59000, 14742008] Large intestinal structure (body structure)
Why HL7 Version 2.3.1? • In 2001 – For First Project – Reasonable, National Standard • For Second Project, proposed HL7 Version 2.5 – Vendor pushback • Vendors using Version 2.3.1 and Version 2 • AP Laboratory community appears to be using this Version • Challenge – Transition to More Robust Formats
RPP Messaging Tables • HL7 Version 2.3.1 • Field Guide Table • OBX Table (CAP Checklist Concepts) • Maps of CAP Checklists Concepts to NAACCR Data Items • Map from Collaborative Stage to CAP Checklist Concepts
Messaging Issues • Versioning • Nested questions • Multiple primaries – message structure • How handle text
Types of Versioning • SNOMED CT – updated every January and July • CAP Cancer Checklists – may be updated every January and July • Date of Checklist – for major changes • SNOMED CT Encoded CAP Cancer Checklists – may be updated every January and July • No mechanism
Melanoma Issue: Nested Concepts • SPECIMEN TYPE [R-00254, 371439000] Specimen type (observable entity) • ___ Excision, ellipse [G-81FD, 396353007] Specimen from skin obtained by elliptical excision (specimen) • ___ Excision, wide [G-81FE, 396354001] Specimen from skin obtained by wide excision (specimen) • ___ Excision, other (specify): ____ [G-81FF, 396355000] Specimen from skin obtained by excision (specimen) (specify): ____ not coded • ___ Re-excision, ellipse [G-8202, 396357008] Specimen from skin obtained by elliptical re-excision (specimen) • ___ Re-excision, wide [G-8203, 396358003] Specimen from skin obtained by wide re-excision (specimen) • ___ Re-excision, other (specify): _____ [G-8201, 396356004] Specimen from skin obtained by re-excision (specimen) (specify): ____ not coded • ___ Lymphadenectomy, sentinel node(s) [R-003AF, 373193000] Lymph node from sentinel lymph node dissection (specimen) • _X_ Lymphadenectomy, regional nodes (specify): _axillary_ [G-8204, 396359006] Lymph node from regional lymph node dissection (specimen) (specify): ____ not coded • ___ Other (specify): ____ not coded • ___ Not specified [G-8110, 119325001] Skin (tissue) specimen (specimen)
CWE With Repeating Segments • _X_ Lymphadenectomy, regional nodes (specify): _axillary_ [G-8204, 396359006] Lymph node from regional lymph node dissection (specimen) (specify): ____ not coded • OBX|1|CWE|371439000^Specimen type (observable entity)^SCT^^^^^SPECIMEN TYPE||396359006^Lymph node from regional lymph node dissection (specimen)^SCT^^^^^^Lymphadenectomy, regional nodes (specify)~^^^^^^^^axillary||||||F
Multiple Specimen/Cancers Scenarios • One specimen to two or more cancers with the same primary site • One specimen to two or more cancers with different primary sites • Many specimens to two or more cancers with the same primary site • Many specimens to two or more cancers with different primary sites
Multiple Primary - Structure MSH/PID/PV1 ORC - Specimen OBR – Part 1 and Worksheet 1 (type) OBX – Heading/Question and Value OBX – " " " " OBX – " " " " OBR – Part 1 and Worksheet 2 (type) OBX – Heading/Question and Value OBX – " " " " OBX – " " " " OBR – Part 3 and Worksheet 3 (type) OBX – Heading/Question and Value OBX – " " " " OBX – " " " "
Incorporate Text • For the transmission of text data, RPP2 will rely upon the NAACCR E-Path transmission standards as noted in NAACCR Volume V
Recommendations • All cancers are not reported via an existing checklist • Need strategy for the remainder • Multiple histology and primary rules may differ • Examine coding rules used by pathologists for consistency with cancer registry rules • Checklists need to be assessed for stage information • Collaborative stage
Recommendations • Cancer registry community needs to evaluate • Expand NAACCR E-Path standards to synoptic • Establish mapping between checklist data items and NAACCR data items • Informatics community needs to assess vocabulary and mapping issues • Establish the question and answer vocabulary
Recommendations • Examine costs associated with synoptic reporting • Cost for pathology lab software (AP LIS) • Cost for SNOMED CT Encoded CAP Checklists • Pathology lab software vendors • Add text fields to synoptic reports • Add drop-down menus for histology codes
Potential • Reduce coding from narrative text • Facilitate the abstracting process • Capture intent of pathologists • Improve rapid case-ascertainment systems • Create more complete case reports • Improve completeness of reporting
An idea whose time has come? • Work through issues of vocabulary and mapping • Work through staging issues • Implement checklists more quickly • Integrate into cancer registry software • Abstract • Rapid Case-Ascertainment
RPP Report • Published on the NPCR web site • www.cdc.gov/cancer/npcr/
Contacts • Ken Gerlach 770-488-3008 kgerlach@cdc.gov • Missy Jamison 770-488-7154 mjamison@cdc.gov • Sharon Winters 412-647-6390 winterssb@upmc.edu • Anil Parwani 412-623-1326 parwaniav@upmc.edu
Ken Gerlach 770-488-3008 kgerlach@cdc.gov Thank you The findings and conclusions in this presentation are those of the author(s) and do not necessarily represent the views of the Centers for Disease Control and Prevention