Download
1 / 15
300 likes | 1.17k Views
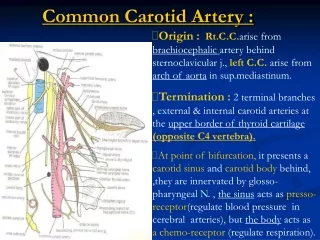
CAROTID DISSECTION. Morning Report July 12, 2010 Ann Isaksen. DEFINITION. Tear in the intimal layers of wall of carotid artery leading to either Intramural Hematoma Aneurysmal dilation of vessel Both Stasis Microemboli Ischemic CVA. Carotid Dissection & CVA.

E N D
CAROTID DISSECTION Morning Report July 12, 2010 Ann Isaksen
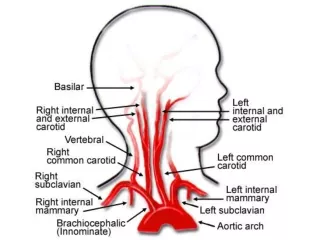
DEFINITION • Tear in the intimal layers of wall of carotid artery leading to either • Intramural Hematoma • Aneurysmal dilation of vessel • Both Stasis Microemboli Ischemic CVA
Carotid Dissection & CVA • Internal carotid artery dissection accounts for up to 25% of ischemic strokes in pts < 45yo. • Dissection can occur Intracranial or Extracranial (Extracranial more common) • Extracranial carotid artery = mean age of 40 years. • Intracranial dissections = aged 20-30 years
SYMPTOMS • Headache, including neck and facial pain, can be constant, instantaneous, gradual, throbbing, or sharp. • Headache is commonly ipsilateral to the dissected artery. • Headache usually precedes a cerebral ischemic event, unlike a headache associated with stroke, which usually follows or accompanies the ischemic event. • Transient episodic blindness, or amaurosis fugax, is caused by decreased blood flow to the retina. • Ptosis with miosis, (partial Horner syndrome). • painful when caused by internal carotid artery dissections. • Neck swelling • Pulsatile tinnitus can occur in up to 25% of patients with dissection of the internal carotid artery. • Decreased taste sensation, or hypoageusia • Focal weakness
OTHER ASSOCIATED FINDINGS • Cranial nerve palsy in up to 12% of patients • Lower cranial nerves affected more often than the facial, trigeminal, and oculomotor nerves. • Cervical bruit • Cervicothoracic seat belt sign, which is ecchymosis to the neck and chest, raises the incidence of cerebrovascular injuries (internal carotid or vertebral) • Cervical spine injuries, maxillofacial trauma, basilar skull fractures • Massive epistaxis • Evidence of near hanging injury or strangulation injury
ASSOCIATED CONDITIONS • Heritable connective-tissue disorders • Ehlers-Danlos syndrome type IV • Fibromuscular dysplasia • Cystic medial necrosis • Marfan syndrome • Autosomal dominant polycystic kidney disease • Osteogenesis imperfecta type I • Oral contraceptives • Hypertension • Neck manipulation or strain
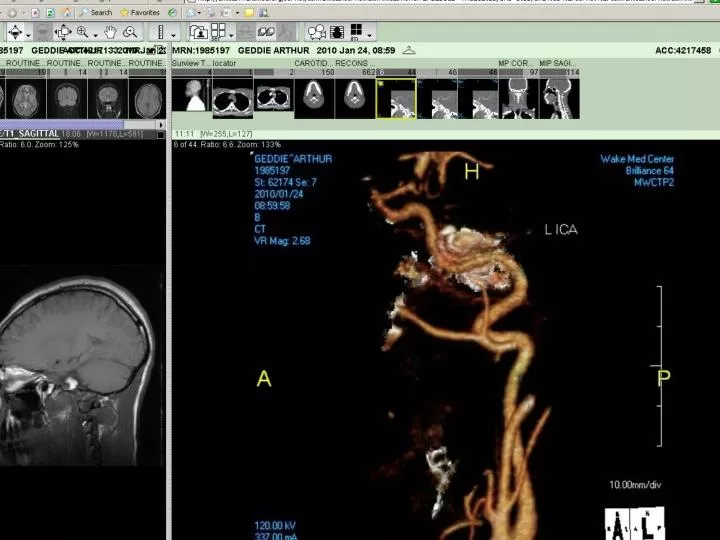
CAROTID CTA • The hallmark of injury to the internal carotid artery is a change in the caliber of the vessel. • CTA is nearly always sufficient to confirm the diagnosis of carotid artery dissection, and even early studies (1996) with CTA achieved 100% sensitivity and specificity with arterial angiography.
MRI/MRA • MRI scans with fat saturation can show intramural blood, and mural expansion, pathological hallmark of dissection • MRA may fail to detect intramural hematoma within the first 24-48 hours after occurrence of carotid artery dissection.12 • Other MRA signs of dissection include • irregular vessel margins, • filling defects, • extravasation of contrast, • vascular occlusion, and • caliber changes of the vessel.
Doppler ultrasonography • DUS has the lowest cost and highest safety profile of all the imaging modalities presented, and reported sensitivities are as high as 96% in diagnosing carotid artery dissections in patients who suffered stroke. • An abnormal blood flow pattern can be appreciated in up to 90% of patients with carotid artery dissection, but the actual site of injury is usually not seen because of limited ability to evaluate past the carotid bulb. • The most common DUS finding in carotid artery dissection is high resistance flow pattern or absence of signal in a totally occluded artery. • However, ultrasound to have a relatively high false-negative rate in patients with carotid artery dissection presenting with Horner syndrome. • Abnormalities found by duplex scanning should always be followed up with another imaging modality.
TREATMENT • Surgery has a limited role in the management of carotid artery dissections • 1st line therapy = Anticoagulation with intravenous heparin followed by warfarin to prevent thromboembolic complications. • Antiplatelet therapy has also been used alone especially when systemic anticoagulation is contraindicated. • Candidates for angioplasty and stent placement include patients with persistent ischemic symptoms despite adequate anticoagulation, patients with contraindication to anticoagulation therapy, iatrogenic dissection during intravascular procedures, and patients with significantly compromised cerebral blood flow.
PROGNOSIS • Carotid dissections generally heal in 3-6mths • If anticoagulation therapy is initiated, this is generally continued for 3-6 months • Target INR should between 2.0 and 3.0. • A follow-up CT-angiogram, Duplex ultrasonography, or other angiographic imaging modalities should be obtained several months after the event to reevaluate the dissection.
REFERENCES • Schievink WI. Spontaneous dissection of the carotid and vertebral arteries. N Engl J Med. Mar 22 2001;344(12):898-906. • Debette S, Leys D. Cervical-artery dissections: predisposing factors, diagnosis, and outcome. Lancet Neurol. Jul 2009;8(7): 668-78. • Cothren CC, Moore EE, Biffl WL, Ciesla DJ, Ray CE Jr, Johnson JL. Anticoagulation is the gold standard therapy for blunt carotid injuries to reduce stroke rate. Arch Surg. May 2004;139(5):540-5
THE END Northern Spotted Owl, Olympic National Park