Download
1 / 28
350 likes | 436 Views
Learn about heart rate variability (HRV) analysis to understand autonomic physiology in healthcare settings. Explore the influence on HRV by intrinsic and extrinsic rhythms, benefits, and clinical correlates.

E N D
Heart Rate Variability for Clinicians Phyllis K. Stein, Ph.D. Research Associate Professor of Medicine and Director, Heart Rate Variability Laboratory Washington University School of Medicine St. Louis, MO
The Big Picture • Heart rate is under both sympathetic (SNS) and parasympathetic (PNS) control. • Rapid fluctuations in heart rate usually reflect PNS control only (respiratory sinus arrhythmia). • Therefore, changes in heart rate over time provide a window onto autonomic physiology. • Analysis of heart rate variability (HRV) quantifies these changes over time.
Parasympathetic Nervous system Heart Rate Cardiac output Blood pressure Renin angiotensin system Sympathetic Nervous system Simplified model of cardiovascular control showing modulation of heart rate by parasympathetic and sympathetic feedback loops
Influences on HRV Extrinsic Rhythms • Activity • Sleep-wake cycle • Eating Meals • Mental Stress • Physical Stress
Influences on HRV Intrinsic Periodic Rhythms • Respiratory sinus arrhythmia • Baroreceptor reflex regulation • Thermoregulation • Neuroendocrine secretion • Circadian rhythms • Sleep stages during the night • Other, unknown rhythms
QuantifyingHRV Approach 1: The Physiologist’s Paradigm HR data collected over short period of time (~5-20 min), with or without interventions, under carefully controlled laboratory conditions. Approach 2: The Clinician’s and the Epidemiologists’s Paradigm Ambulatory Holter Recordings collected over 24-hours or less, usually on outpatients.
Quantifying HRV Approach 1: How much variability is there? Time Domain and Geometric Analyses Approach 2: What are the underlying rhythms? What physiologic process do they represent? How much power does each underlying rhythm have? Frequency Domain Analysis Approach 3: How much complexity or self-similarity is there? Non-Linear Analyses
Time Domain HRV • Calculated from normal-to-normal interbeat (N-N) intervals • SDNN-Standard deviation of N-N intervals in ms (Total HRV) • SDANN-Standard deviation of 5- min mean values of N-Ns for each 5 minute interval in ms (Circadian HRV) • Both reflect “longer-term” HRV
Time Domain HRV • SDNNIDX-Average of standard deviations of N-Ns for each 5 min interval in ms (Combined sympathetic and parasympathetic HRV) • Reflects “intermediate-term” HRV • AVGNN-Average of N-N intervals in ms • Equivalent to heart rate of normal-to-normal beats. (HR=60,000/AVNN)
Time Domain HRV • Calculated from differences between successive N-N intervals • rMSSD-Root mean square of successive differences of N-N intervals in ms • pNN50-Percent of successive N-N differences >50 ms Referred to as “short-term” HRV and reflect parasympathetic influence on heart rate
Frequency Domain HRV • Based on autoregressive techniques or fast Fourier transform (FFT). • Partitions the total variance in heart rate into underlying rhythms that occur at different frequencies. • These frequencies can be associated with different intrinsic, autonomically-modulated periodic rhythms.
What are the Underlying Rhythms? One rhythm 5 seconds/cycle or 12 times/min 5 seconds/cycle= 1/5 cycle/second 1/5 cycle/second= 0.2 Hz
What are the Underlying Rhythms? Three Different Rhythms High Frequency = 0.25 Hz (15 cycles/min Low Frequency = 0.1 Hz (6 cycles/min) Very Low Frequency = 0.016 Hz (1 cycle/min)
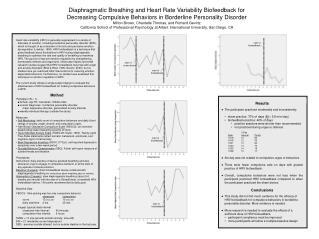
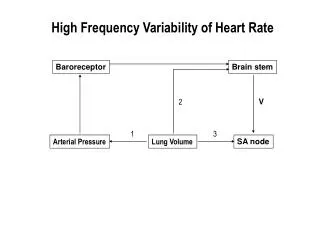
What are the Underlying Rhythms in the Heart Rate Signal? • High frequency band (HF) • At respiratory frequencies (9-24 cycles/minute) • PNS influences on HR • Low frequency band (LF) At Mayer wave frequencies~every 8- 10 sec frequency Baroreceptor, SNS, PNS influences on HR
What are the Underlying Rhythms in the Heart Rate Signal? • Very low frequency band (VLF) At ~every 20 sec-every 5 min frequency Reflects vasomotor changes, thermoregulatory, possibly PNS influences on HR • Ultra low frequency power band (ULF) • At >every 5 min to once in 24 hours • Reflects circadian, neuroendocrine, activity, other unknown rhythms
LF peak HF peak 0 0.20 Hz 0.40 Hz 24-hour average of 2-min power spectral plots in a healthy adult
Non-Linear HRV • Non-linear HRV characterize the structure of the HR time series, i. e., is it random or self-similar. • Increased randomness of the HR time series is associated with worse outcomes in cardiac patients.
Non-Linear HRV • Most commonly used measure of randomness is the short-term fractal Scaling exponent (DFA1). Decreased DFA1 increased randomness of the HR. • Another index is power law slope, a measure of longer term self-similarity of HR. Decreased slope worse outcome. • Normal DFA1 is about 1.1. DFA1<0.85 is associated with higher risk.
Clinical Correlates of Decreased HRV • Inducible VT and VF • Risk of Sudden Cardiac Death • Increased mortality post-MI • Congestive heart failure • Poorer survival in CHF • COPD
Clinical Correlates of Decreased HRV • Diabetic neuropathy • Alcoholic neuropathy • Post cardiac transplant • Depression • Susceptibility to SIDS • Poor survival in premature babies • Increased mortality in population studies
Pitfalls in Understanding HRV • HRV reflects phasic not tonic modulation of HR and cannot measure autonomic tone, just modulation of HR. • HRV is a “black box.” Decreased HRV can mean decreased autonomic input or decreased cardiac responsiveness. • HRV cutpoints for risk stratification best established in immediate post-MI period.
Pitfalls in Understanding HRV • Association is not causation • Endurance athletes have high HRV. • Does exercise training cause increased HRV, or are people with high HRV more suited to endurance exercise? • HRV can be exaggerated by increased randomness, which is not a truly normal sinus rhythm despite the normal appearance of the ECG.
Clinical Implications • Normal HRV is a good negative risk stratifier. • Patients with preserved HRV (SDNN>100 ms) are low risk in the absence of other significant risk factors. • Sensitivity and specificity of decreased HRV (SDNN<70 ms) for immediate post-MI is about 30%.
How Can HRV Be Increased? • Medications • Beta-blockers • ACE inhibitors in CHF • Digoxin? • Ventricular resynchronization therapy • Cardiac rehab?
How Can HRV Be Increased? • Lifestyle modifications: • Smoking cessation • Weight loss • Exercise • Stress management • Lipid lowering? • Glycemic control
Final Thoughts • Analysis of HRV is a non-invasive method for identifying abnormalities in cardiac autonomic modulation. • Decreased HRV by itself is not sufficient to risk stratify patients, e.g. for AICD implantation, but HRV in combination with other risk stratifiers improves risk stratification.
Final Thoughts • Normal HRV identifies patients at lower risk for events. • HRV cutpoints are population-specific and have not been fully elucidated. • It now appears that decreased HRV and increased randomness of HR are independently associated with higher risk.