Download
1 / 14
140 likes | 151 Views
Dr. Shakti Swaroop is a dedicated ankle pain and swelling orthopedic surgeon & best foot and ankle specialist in Bhubaneswar, Odisha

E N D
Posterior tibial tendon dysfunction (PTTD) : A progressive collapsing foot deformity
Flat foot ( Introduction) • Flat foot is present with 54% children < 3 years but only 24% with children beyond 6 years • Normal medial longitudinal arch may take 10 years to develop. • Flexible flat foot have a tendency to progress into adulthood • When progress into adulthood they present as tibialis posterior tendon insufficiency or PTTD. • When not treated early progressively collapse to severe arthritis of foot • New nomenclature 2020 Progressive collapsing foot deformity(PCFD)
What is flat foot? • Absence of normal medial longitudinal arch in foot • Prevalent in almost 20 - 25 % of adults ( females ) • Flexible or rigid ( depends on flexibility of joints) • Symptomatic or asymptomatic ( fatigue pain/ arthritis/ tendinoapthy)
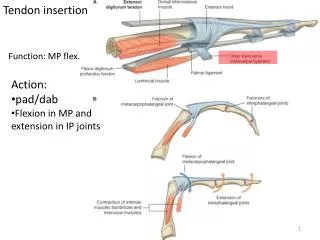
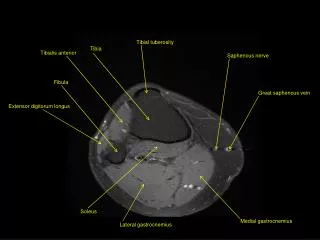
Arches of the foot • Medial longitudinal arch • Lateral longitudinal arch • Transverse metatarsal arch
Medial longitudinal arch • Formed by a bony arch and a tie arch tying them together • The bones involved are calcaneum , talus and medial 3 cuneiforms and medial three metatarsals • Ligaments – deltoid ligament Sprint ligament, plantar aponeurosis • Muscles – Tibialis posterior Tibialis anterior , Flexor hallucis longus
PTTD a clinical spectrum ( Progressive) • Posterior tibial tendon dysfunction should be viewed as a syndrome in which there is a spectrum of clinical presentations. • This spectrum ranges from patients with recent onset (synovitis can create pain, yet motor function is preserved) • To patients with long-standing disease (marked collapse of the hindfoot and midfoot is present and motor function is absent). • Completing the progressive collapse of the arch leading to a flat foot
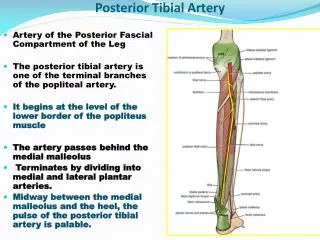
Pathophysiology of PTTD (Progressive collapse) • With growth stress on the tibialis posterior muscle increases ( Mechanical disadvantage due to hypermobile subtalar joint ) • Passes at an acute angle behind the medial malleolus • Lies medial and behind the talocalcaneal ( subtalar) joint • Avascular zone behind the medial malleolus (4-6 cm) • Translation is 1-2 cm so inherent elasticity is less • Fibrocartilage tissue covering at the medial malleolus - less stretchable • Constricted within the flexor retinaculum sheath & bone
Why the Tibialis posterior fails? • Due to the mechanical disadvantage • Lack of tensile strength • Avascular zone at the site of maximum stress • Once inflammation starts collagen degenerates • Longitudinal tears start • Eventually tendon fails & stresses the spring ligament
Progression after tibialis posterior fails • The hindfoot goes into valgus due to unopposed action of peroneus group • Increased stress on spring ligament causes the talonavicular joint to sag • Talus head subluxates inferiorly and medially ( talar head uncover age) • Spring ligament fails and midfoot collapses
Predisposing factors • Childhood flat foot ( Familial ) • Females • Ligamentous laxity • Diabetes • Steroids • Obesity • Inflammatory diseases • Overactivity stress
Clinical presentation • Middle aged obese lady presenting with medial side ankle pain • Painful to walk and climb stairs • Pain gradually also effects lateral side • Swelling appears late pitting in nature • Eventually hindfoot and midfoot becomes painful and arthritic
Single Heel rise test Inspection from behind for heel valgus Uncoverage of TN joint Subfibular impingement Single Heel rise test ( Failure to invert ) Heel valgus
Treatment @ Stage 2 (joints are preserved) • Surgical correction is required to prevent its further progression • Mechanical correction and substituting the posterior tibial tendon with Flexor Digitorum longus (FDL Transfer) • Mechanical correction achieved by medial sliding calcaneal osteotomy / Evans osteotomy • Augmentation or reconstruction of the spring ligament
Thank you Dr Shakti Swaroop Sr. Consultant Orthopaedic Surgeon Foot and Ankle specialist www.footankleortho.com