Download
1 / 57
570 likes | 598 Views
Disorders of Endocrine glands Dr. Zainab Sajid Al- Shimmari. HYPOTHYROIDISM: Thyroid Disorders: I-Congenital Hypothyroidism.

E N D
Disorders of Endocrine glands Dr. ZainabSajid Al-Shimmari
HYPOTHYROIDISM: Thyroid Disorders: I-Congenital Hypothyroidism. 1- Hypothyroidism in the infant may result from a congenital lack of the thyroid gland or from abnormal biosynthesis of thyroid hormone or deficient TSH secretion. With congenital lack of the thyroid gland, the infant usually appears normal and functions normally at birth because hormones have been supplied in utero by the mother.
2-The manifestations of untreated congenital hypothyroidism are referred to as cretinism. However, the term does not apply to the normally developing infant in whom replacement thyroid hormone therapy was instituted shortly after birth. 3-Thyroid hormone is essential for normal brain development and growth, almost half of which occurs during the first 6 months of life. If untreated, congenital hypothyroidism causes mental retardation and impairs growth.
4-The fetal and infant thyroids are sensitive to iodine excess. Iodine crosses the placenta and mammary glands and is readily absorbed by infant skin. 5-Transient hypothyroidism may be caused by maternal or infant exposure to substances such as povidone-iodine used as a disinfectant.
II-Acquired Hypothyroidism and Myxedema 1-Hypothyroidism in older children and adults causes a general slowing down of metabolic processes and myxedema. 2-Myxedema implies the presence of a non pitting mucous type of edema caused by an accumulation of a hydrophilic mucopolysaccharide substance in the connective tissues throughout the body.
3-The hypothyroid state may be mild,with only a few signs and symptoms, or it may progress to a life-threatening condition called myxedematous coma. It can result from destruction or dysfunction of the thyroid gland (i.e., primary hypothyroidism), or it can be a secondary disorder caused by impaired pituitary function or a tertiary disorder caused by a hypothalamic dysfunction.
Causes 1-Primary hypothyroidism is much more common than secondary (and tertiary) hypothyroidism. It may result from thyroidectomy or ablation of the gland with radiation. Certain goitrogenic agents, such as lithium carbonate and the anti thyroid drugs in continuous dosage can block hormone synthesis and produce hypothyroidism with goiter. 2-Large amounts of iodine ingestion also can block thyroid hormone production and cause goiter.
.3- in persons with autoimmune thyroid disease. Iodine deficiency, which can cause goiter and hypothyroidism. 4-The most common cause of hypothyroidism is Hashimoto’s thyroiditis, an autoimmune disorder in which the thyroid gland may be totally destroyed by an immunologic process. It is the major cause of goiter and hypothyroidism in children and adults. 5-The transit hyperthyroid state is caused by leakage of preformed thyroid hormone from damaged cells of the gland.
This is the normal appearance of the thyroid gland on the anterior trachea of the neck. The thyroid gland has a right lobe and a left lobe connected by a narrow isthmus. The normal weight of the thyroid is 10 to 30 grams. It cannot easily be palpated on physical examination
Normal thyroid seen microscopically consists of follicles lined by a an epithelium and filled with colloid. The follicles vary some what in size.
This symmetrically small thyroid gland demonstrates atrophy. This patient was hypothyroid. This is the end result of Hashimoto's thyroiditis. Initially, the thyroid is enlarged and there may be transient hyperthyroidism, followed by aeuthyroid state and then hypothyroidism with eventual atrophy years later.A
Manifestations. 1-The myxedema is most obvious in the face and other superficial parts, it also affects many of the body organs and is responsible for many of the manifestations of the hypothyroid state . 2-The hypometabolic state associated with hypothyroidism is characterized by a gradual onset of weakness and fatigue,a tendency to gain weight despite a loss of appetite,and cold intolerance.
3- As the condition progresses, the skin becomes dry and rough and acquires a pale yellowish cast,which primarily results from carotene deposition, and the hair becomes coarse and brittle. 4-There can be loss of the lateral one third of the eyebrows. 5-Gastrointestinal motility is decreased, producing constipation, flatulence, and abdominal distention.
6- Nervous system involvement is manifested in mental dullness, lethargy, and impaired memory. 7-As a result of myxedematous fluid accumulation, the face takes on a characteristic puffy look, especially around the eyes. The tongue is enlarged. Pericardial or pleural effusion may develop. 8-Mucopolysaccharide deposits in the heart cause generalized cardiac dilatation, bradycardia, and other signs of altered cardiac function.
HYPERTHYROIDISM Thyrotoxicosis is the clinical syndrome that results when tissues are exposed to high levels of circulating thyroid hormone. thyrotoxicosis is due to hyperactivity of the thyroid gland, or hyperthyroidism. Causes. 1-The most common cause of hyperthyroidism is Graves’ disease, which is accompanied by ophthalmopathy (or dermopathy) and diffuse goiter.
2- Multi nodular goiter, adenoma of the thyroid, and, occasionally, ingestion of excessive thyroid hormone. 3-Iodine-containing agents can induce hyperthyroidism as well as hypothyroidism. Thyroid crisis, or storm, is an acutely exaggerated manifestation of the thyrotoxic state.
This diffusely enlarged thyroid gland is somewhat nodular. This patient was euthyroid. This represents the most common cause for an enlarged thyroid gland and the most common disease of the thyroid--a nodular goiter.
Here is another follicular neoplasm (a follicular adenoma histologically) that is surrounded by a thin white capsule. It is sometimes difficult to tell a well-differentiated follicular carcinoma from a follicular adenoma. Thus, patients with follicular neoplasms are treated with subtotal thyroidectomy just to be on the safe side.
Manifestations. 1- The manifestations are related to the increase in oxygen consumption associated with the hypermetabolic state as well as to the increase in sympathetic nervous system activity that occurs. 2-The fact that many of the signs and symptoms of hyperthyroidism resemble those of excessive sympathetic nervous system activity suggests that thyroid hormone may heighten the sensitivity of the body to the catecholamines or that it may act as a pseudocatecholamine.
3-Weight loss is common despite a large appetite. 4-tachycardia, palpitations, shortness of breath, excessive sweating, muscle cramps, and heat intolerance. The person appears restless and has a fine muscle tremor. 5- Even in persons without exophthalmos (bulging of the eyeballs seen in ophthalmopathy),there is an abnormal retraction of the eyelids and infrequent blinking such that they appear to be staring.
Graves’ Disease. 1-Graves’ disease is a state of hyperthyroidism, goiter, and ophthalmopathy (or, less commonly, dermopathy).The onset usually is between the ages of 20 and 40 years,and women are five times more likely to develop the disease than men. 2- Graves’ disease is an autoimmune disorder characterized by abnormal stimulation of the thyroid gland by thyroid-stimulating antibodies (thyroid-stimulating immunoglobulins[TSI]) that act through the normal TSH receptors. The disease is associated with human leukocyte antigen (HLA and a familial tendency is evident.
At high power, the tall columnar thyroid epithelium with Grave's disease lines the hyperplastic infoldings into the colloid. Note the clear vacuoles in the colloid next to the epithelium where the increased activity of the epithelium to produce increased thyroid hormone has led to scalloping out of the colloid
3-The ophthalmopathy, which occurs in up to one third of persons with Graves’ disease, is thought to result from a cytokine-mediated activation of fibroblasts in orbital tissue behind the eyeball. 4-Humoral autoimmunity also is important; an ophthalmic immunoglobulin may exacerbate lymphocytic infiltration of the extra ocular muscles.
5-The ophthalmopathy of Graves’ disease can cause severe eye problems, including paralysis of the extra ocular muscles ;involvement of the optic nerve, with some visual loss;and corneal ulceration because the lids do not close over the protruding eyeball (due to the exophthalmos).
Adrenal gland disorders. Congenital Adrenal Hyperplasia. 1-Congenital adrenal hyperplasia (CAH), or the adrenogenital syndrome, describes a congenital disorder caused by an autosomal recessive trait in which a deficiency exists in any of the enzymes necessary for the synthesis of cortisol.
2-A common characteristic of all types of CAH is a defect in the synthesis of cortisol that results in increased levels of ACTH and adrenal hyperplasia. The increased levels of ACTH over stimulate the pathways for production of adrenal androgens. Mineral corticoids may be produced in excessive or insufficient amounts, depending on the precise enzyme deficiency.
3-Infants of both sexes are affected. A- Males seldom are diagnosed at birth unless they have enlarged genitalia or lose salt and manifest adrenal crisis. B-In female infants, an increase in androgens is responsible for creating the virilization syndrome of ambiguous genitalia with an enlarged clitoris, fused labia, and urogenital sinus. C- In male and female children,other secondary sex characteristics are normal, and fertility is unaffected if appropriate therapy is instituted.4-The two most common enzyme deficiencies are21-hydroxylase and 11-β-hydroxylase deficiency.
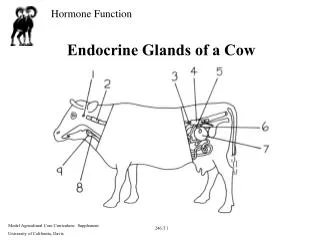
Here are normal adrenal glands. Each adrenal weighs from 4 to 6 grams
The pair of adrenals in the center are normal. Those at the top come from a patient with adrenal atrophy (with either Addison's disease or long-term corticosteroid therapy). The adrenals at the bottom represent bilateral cortical hyperplasia. This could be due to a pituitary adenoma secreting ACTH (Cushing's disease), or Cushing's syndrome from ectopic ACTH production, or idiopathic adrenal hyperplasia.
Clinical manifestations : 1-A spectrum of 21-hydroxylase deficiency states exists,ranging from simple virilizing CAH to a complete salt losing enzyme deficiency. A-Simple virilizing CAH impairs the synthesis of cortisol, and steroid synthesis is shunted to androgen production. Persons with these deficiencies usually produce sufficient aldosterone or aldosterone intermediates to prevent signs and symptoms of mineralocorticoid deficiency.
B-The salt-losing form is accompanied by deficient production of aldosterone and its intermediates. This results in fluid and electrolyte disorders after the fifth day of life (including hyponatremia,hyperkalemia, vomiting, dehydration, and shock). 2-The 11-β-hydroxylase deficiency is rare and manifests a spectrum of severity. Affected persons have excessive androgen production and impaired conversion of11-deoxycorticosterone to corticosterone The over production of 11-deoxycorticosterone, which has mineral corticoid activity, is responsible for the hypertension that accompanies this deficiency.
ADRENAL CORTICAL INSUFFICIENCY There are two forms of adrenal insufficiency: primary and secondary. I-Primary Adrenal Cortical Insufficiency. The primary adrenal insufficiency,now called Addison’s disease.The use of this term is reserved for primary adrenal insufficiency in which adrenal cortical hormones are deficient and ACTH levels are elevated because of lack of feedback inhibition.Addison’s disease is a relatively rare disorder in which all the layers of the adrenal cortex are destroyed.
Causes 1-Autoimmune destruction is the most common cause of Addison’s disease in the United States. 2- Before 1950, tuberculosis was the major cause of Addison’s disease in the United States. 3-Rare causes include metastatic carcinoma, fungal infection( histoplasmosis),cytomegalovirus infection, amyloid disease,and hemochromatosis. 4-Bilateral adrenal hemorrhage may occur in persons taking anticoagulants, during open heart surgery, and during birth or major trauma. 5-Acquired immunodeficiency syndrome, in which the adrenal gland is destroyed by a variety of infectious agents.
Manifestations. 1-the manifestations of adrenal insufficiency usually do not become apparent until approximately 90% of the gland has been destroyed. These manifestations are related primarily to mineral corticoid deficiency, glucocorticoid deficiency, and hyper pigmentation resulting from elevated ACTH levels. 2-lack of the adrenal androgens exerts few effects in men because the testes produce these hormones, women have sparse axillary and pubic hair.
3-Mineralocorticoid deficiency causes increased urinary losses of sodium, chloride, and water, along with decreased excretion of potassium. The result is hyponatremia, loss of extracellular fluid, decreased cardiac output, and hyperkalemia. 4-There may be an abnormal appetite for salt. Orthostatic hypotension is common. Dehydration, weakness,and fatigue are common early symptoms. If loss of sodium and water is extreme, cardiovascular collapse and shock.
5-Because of a lack of glucocorticoids, the person with Addison’s disease has poor tolerance to stress. This deficiency causes hypoglycemia, lethargy, weakness, fever, and gastrointestinal symptoms such as anorexia, nausea, vomiting,and weight loss. 6-Hyperpigmentation results from elevated levels of ACTH. The skin looks bronzed or suntanned in exposed and unexposed areas .The gums and oral mucous membranes may become bluish-black. hyper pigmentation occurs in more than 90% of persons with Addison’s disease and is helpful in distinguishing the primary and secondary forms of adrenal insufficiency.
II-Secondary Adrenal Cortical Insufficiency. Secondary adrenal insufficiency can occur as the result of hypopituitarism or because the pituitary gland has been surgically removed. Tertiary adrenal insufficiency results from a hypothalamic defect. However, a far more common cause than either of these is the rapid withdrawal of glucocorticoids that have been administered therapeutically.
CUSHING’S SYNDROME The term Cushing’s syndrome refers to the manifestations of hypercortisolism from any cause. Three important forms of Cushing’s syndrome result from excess glucocorticoid production by the body. I-pituitary form which results from excessive production of ACTH by a tumor of the pituitary gland. This form of the disease was the one originally described by Cushing; therefore; it is called Cushing’s disease.
II- Adrenal form, caused by a benign or malignant adrenal tumor. III- Ectopic Cushing’s,caused by a non pituitary ACTH-secreting tumor. Certain extra pituitary malignant tumors such as small cell carcinoma of the lung may secrete ACTH and produce Cushing’s syndrome. VI-Cushing’s syndrome also can result from long-term therapy with one of the potent pharmacologic preparations of glucocorticoids; this form is called iatrogenic Cushing’s syndrome.
This adrenal gland removed surgically in a patient with Cushing's syndrome has been sectioned in half to reveal an adenoma. Some remaining atrophic adrenal is seen at the right. The adenoma is composed of yellow firm tissue just like adrenal cortex. This neoplasm is well-circumscribed. Histologically, it is composed of well-differentiated cells resembling cortical fasciculata zone. It is benign
This is a large adrenal cortical carcinoma which is displacing the left kidney downward. Such neoplasms are usually functional (secreting corticosteroids or sex steroids). They have a poor prognosis.
Manifestations of Cushing’s syndrome. 1- Altered fat metabolism causes a peculiar deposition of fat characterized by a protruding abdomen; subclavicular fat pads or “buffalo hump” on the back; and around, plethoric “moon face” .2- There is muscle weakness, and the extremities are thin because of protein breakdown and muscle wasting.