Download
1 / 74
860 likes | 1.48k Views
Inflammatory Disorders of the Heart. infection of endocardial surface of heart. Endocarditis Pericarditis Myocarditis. focal or diffuse inflammation of myocardium. inflammation of pericardial sac (pericardium ).

E N D
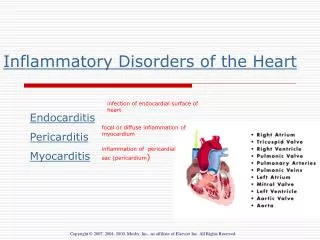
Inflammatory Disorders of the Heart infection of endocardial surface of heart Endocarditis Pericarditis Myocarditis focal or diffuse inflammation of myocardium inflammation of pericardial sac (pericardium)
Endocarditis: precipitated by bacteria/fungal infection; potential death from emboli and valvular disturbance Myocarditis: virus, toxin or autoimmune response damage heart muscle > lead to cardiomyopathy and death! Pericarditis: Bacterial, fungal or viral infection affect visceral and parietal pericardium; restrict heart pumping action> lead to cardiac tamponade and death!
Layers of the Heart Layers of heart muscle and pericardium; section of heart wall shows fibrous pericardium, parietal and visceral layers of serous pericardium (with pericardial sac between them), myocardium, and endocardium- Fig. 37-1
Infective Endocarditis(Click to access YOUTube video) • Infection of inner layer of heart- usually affects cardiac valves • Was almost always fatal until development of penicillin • 15,000 cases diagnosed in US each year
A- Aortic Valve B- Mitral Valve C- Tricuspid Valve - Pulmonary Valve
A&P Review- Blood enters right atrium and moves through _______ into right ventricle. Blood then moves from right ventricle into pulmonary artery via _________. • After entering left atrium via pulmonary veins, blood moves through the _____ into left ventricle. • Finally, it travels through the _____ and out of heart A- Aortic Valve B- Mitral Valve C- Pulmonary Valve D- Tricuspid Valve A- Aortic Valve B- Mitral Valve C- Pulmonary Valve D- Tricuspid Valve
Risk Factors- endocarditis • Hx of rheumatic fever or damaged heart valve • Prior history of endocarditis • Invasive procedures- (introduce bacteria into blood stream) dental,gyne, etc. • Recent Dental Surgery • Permanent Central Venous Access • IV drug users • Valve replacements
Classification • Subacute form (subacute bacterial endocarditis-SBE) • Gradual onset; longer clinical course • Caused by enterococci • Usually those with damaged valves • Acute form • Shorter clinical course • Abrupt onset • Usually those with healthy valves • Usually caused by staph aureus • *Classify by cause as IVBA; prosthetic valve endocarditis (PVE), fungal endocarditis
Causative Organisms • Most common causative organism • Streptococcus viridans • Staphylococcus aureus • Viruses • Fungi
Etiology and Pathophysiology • Key -Blood turbulence within heart allows causative agent to infect previously damaged valves or other endothelial surfaces • Principal risk factors • Prior endocarditis • Prosthetic valves • Acquired valvular disease • Cardiac lesions
When valve damaged, blood > slowed down > forms clot. • Bacteria > into blood stream • Bacterial or fungal vegetative growths deposit on normal or abnormal heart valves • Infection of innermost layers of heart may occur in people with: • congenital and valvular heart disease • history of rheumatic heart disease • normal valves with increased amounts of bacteria
Bacterial Endocarditis of Mitral Valve Bacterial endocarditis of mitral valve. Valve covered with large, irregular vegetations (note arrow). From text
Etiology and Pathophysiology • Vegetation • Fibrin, leukocytes, platelets, and microbes • Adhere to valve or endocardium • Embolization of portions of vegetation into circulation
Sequence of Events in Infective Endocarditis (view carefully) Fig. 37-3
Clinical Manifestations • Nonspecific • *Fever in 90% of patients • Chills • Weakness • Malaise • Fatigue • Anorexia • *Murmur
Clinical Manifestations • Subacute form • Arthralgias • Myalgias • Back pain • Abdominal discomfort • Weight loss • Headache • Clubbing of fingers
Clinical Manifestations • Vascular manifestations • Splinter hemorrhages in nail beds • Petechiae * most common • Osler’s nodes on fingers or toes *painful • Janeway’s lesions on palms or soles • Roth’s spots • *Murmur in most patients • Heart failure in up to 80% with aortic valve endocarditis • *Manifestations secondary to embolism
Sites of emboli due to infective endocarditis (AKA metastic infections)-site determined by location of original lesion
Osler’s nodes Janeway lesions Splinter hemorrhages Roth spots
Osler’s nodes- painful, red or purple pea-sized lesions on toes and fingertips • Splinter hemorrhages- black longitudinal streaks on nail beds • Janeway lesions-flat, painless, small, red spots on palms and soles • Roth spots- hemorrhagic retinal lesions
Diagnostic Studies • History • Recent dental, urologic, surgical, or gynecological procedures • Heart disease; onset *new heart murmur • Recent cardiac catheterization • Skin, respiratory, or urinary tract infection • Laboratory tests • Blood cultures (if temp above 101, typically do 2 sets) • WBC with differential • ESR, CRP • Echocardiography- TEE best- see vegetations • Chest x-ray 1) Vegetations on mitral valve 2) Vegetations on aortic Valce
Collaborative Care • Prophylactic treatment for patients having (see prevention) • Removal or drainage of infected tissue • Renal dialysis • Ventriculoatrial shunts • Antibiotic administration • Monitor antibiotic serum levels (peak & trough) • Subsequent blood cultures • Renal function monitored • BUN, Creatinine
Collaborative Care • Antibiotic therapy cont • IV for 2-8 weeks • *Maybe oral meds if not good candidate for IV and can identify and treat specific causative organism • Fungal and prosthetic valve endocarditis • Responds poorly to antibiotics • Valve replacement- adjunct procedure • Fever • Comfort with ASA, Ibuprofen etc
Collaborative Care • Surgical/Therapeutic/Nursing • Early valve replacement. • Complete bed rest –only if temp remains elevated or signs HF • Overall goals • normal or baseline cardiac function • performance of activities of daily living (ADLs) without fatigue • Antibiotic therapy cont
Nursing Diagnoses • Risk for Imbalanced Body Temperature-Hyperthermia • Risk for Ineffective Tissue Perfusion-emboli • Risk for decreased cardiac output • Ineffective Health Maintenance • Deficient knowledge
Complications • Emboli (50% incidence) • Right side- pulmonary emboli (esp. with IV drug abuse- Why??) • Left side-brain, spleen, heart, limbs,etc • CHF-check edema, rales, VS • Arrhythmias- A-fib • Death .
Collaborative Care • Priority Teaching • Signs/symptoms of life-threatening complications of IE, as cerebral emboli, HF etc. • Monitor fever (chronic or intermittent)- sign that drug therapy ineffective • Monitor lab data, blood cultures- determine effectiveness of antibiotic therapy • *Critical-prophylactic antibiotic therapy prior to ANY invasive procedure - see later slide)
Collaborative Care • Priority Teaching/nursing care • Stress need to avoid infectious people • Avoidance of stress and fatigue • Manage rest, hygiene, nutrition • Assessment of nonspecific manifestations • Monitor laboratory data • Monitor patency of IV • Teach reduction measures dec risk infection • Stress follow-up care
Collaborative Care • Eliminate risk factors • Patient teaching • Penicillin prophylaxis • Recent change Guidelines (not all require prophylaxis) • if prosthetic valve • History of endocarditis • Certain congenital heart defects • Heart transplant recipients- • Removal/drainageinfected tissue • Renal dialysis • Ventriculoatrial shunts • *see tab 37-3&4 • TABLE 37-3 SITUATIONS SeeREQUIRING ANTIBIOTIC PROPHYLAXIS TO PREVENT ENDOCARDITIS • Oral • Dental manipulation involving or periapical region of teeth • Dental manipulation involving perforation of oral mucosa • Dental extractions/dental implants • Prophylactic teeth cleaning with anticipated bleeding • Respiratory • Respiratory tract incisions (e.g., biopsy) • Tonsillectomy/adenoidect • GI/GU • Presence wound infection • Presence UTI
Risk Stratisfication for IE High Risk- • Mechanical prosthetic heart valve • Natural prosthetic heart valve • Prior infective endocardititis • Valve repair with prosthetic material • Most congenital heart diseases Moderate Risk- • Valve repair without prosthetic material • Hypertrophic cardiomyopathy • Mitral valve prolapse with regurgitation • Acquired valvular dysfunction Low Risk- • Innocent heart murmurs • Mitral valve prolapse without regurgitation • Coronary artery disease • People with pacemakers/ defibrillators • Prophylactic antibiotics are generally recommended only for people in the “High Risk” category
Pericarditis(Click to access YouTube video) • Pericarditis • inflammation of pericardium, thin, fluid-filled sac surrounding heart. • Can cause severe chest pain especially upon taking a deep breath) • Shortness of breath; hear pericardial friction rub.
Etiology/Pathophysiology • Pericarditis due to • Bacterial, fungal or viral infection infectious) • Non-infectious as uremia • Hypersensitive/autoimmune as Dresslers syndrome • Heart loses natural lubrication(10-15 ml serous fluid); layers roughen and rub • Inflammatory response>lymphatic fluid build-up- • if sudden > cardiac tamponade- • Pericardial Effusion- usually 250ml before show on x-ray-Can have 1000ml (danger!)
Fig. 37-4 Acute pericarditis. Note shaggy coat of fibers covering surface of heart.
Risk Factors/pericarditis • Be Acute or Chronic • Infectious, non-infections or hypersensitive/autoimmune causes • Acute-48=72 hrs post Mi or late-post MI (Dressler’s syndrome)-4-6 wks • Secondary to chemo and cancer • Secondary to uremia in renal failure-40-50% of pts will develop • Trauma or cardiac surgery • If chronic disorder-pericardium >rigid
Clinical Manifestations • Inflammation and pain • Pericardial friction rub-(click to hear) diaphragm at LL sternal, lean forward, listen at inspiration • Fever • Substernal, sharp, pleuritic chest pain • Inc. with coughing, breathing, turning, lying flat • Dec. with sitting up and leaning forward • Referred to trapezius muscle • Dyspnea
Complications of Pericarditis • Pericardial Effusion • Cardiac Tamponade
Pericardial Effusion(YouTubeVideo) • Can occur rapidly or slowly • Pulmonary compression-cough, dyspnea, and tachypnea • Phrenic nerve art sounds distant, muffled • *Slow build-up; no immediate effects; if rapid>compression of heart >tamponade!
Cardiac Tamponade • Compression of heart • Occur acutely (trauma) or sub-acutely (malignancy) • Symptoms- chest pain, confusion, anxious, ^ CVP, restless, muffled heart sounds • Later- tachypnea, tachycardia, and dec. CO, NVD and pulsus paradoxus • With slow onset dyspnea may be only symptom • If rapid compression-Medical Emergency
PERICARDIUM CARDIAC TAMPONADE Original heart size Excess pericardial fluid
Definition- a decrease in systolic BP with inspirations that is exaggerated in cardiac tamponade
Collaborative Care-Pericarditis, Pericardial Effusion, Cardiac Tamponde • Diagnostic Tests • Medications • Surgical/Therapeutic Interventions • Nursing Diagnosis/Interventions
Diagnostic Tests- to R/O • CBC-inc. WBC, ESR, and CRP • Cardiac Enzymes- inc. but not as much as with MI • *EKG- diffuse St elevation *important to different from MI changes (acute pericarditis) • Echo- for wall movement • CXR; Doppler imaginga • CT or MRI- for pericardial effusion • Pericardiocentesis fluid- determine cause; treat cardiac tamponade