Download
1 / 47
470 likes | 600 Views
Learn about the various genetic and environmental factors contributing to CNS malformations like microcephaly and spina bifida. Discover the diagnosis and management options available for these conditions.

E N D
The incidence of malformations is higher in children with - IUGR and multiple pregnancies • The same anomaly may occur as a result of genetic or environmental causes
Etiology Genetic factors Forms of microcephaly inherited as AR Sex-linked variety of hydrocephalus Hereditary congenital facial paralysis AD Some anomalies have a high risk of recurrence within families Inborn errors of metabolism Cytogenetic abnormalities Most important group are the trisomies( e.g Down Syndrome) Translocations, deletions Maternal age Maternal infections (rubella, CMV)
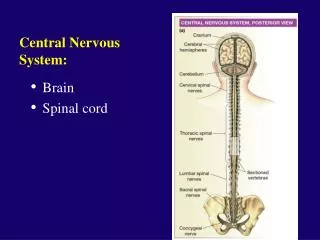
Neural tube defects - Most congenital anomalies of CNS and result from failure of the neural tube to close spontaneously between the 3rd and 4th wk in utero development
Anencephaly • Complete absence of the cerebral hemispheres • Residue of brainstem can be identified • Females > males • Additional anomalies - folding of ears - cleft palate - congenital heart defects • Most of the patients die within several days of birth • 50% of cases have associated polyhydramnios • Genetic basis,low socioeconomic status,nutritional and vitamin deficiency, toxic factors
Encephalocele and cranial meningocele - Protrusion of brain or meninges through a cranial defect - Most frequent in the occipital region - Genetic and environmental factors may be of etiologic importance - Increased risk for hydrocephalus,chiari malformation and Dandy Walker Syndrome - May be completely covered with skin -Risk for visual problems - microcephaly - mental retardation - seizures - Cranial meningocel-generally good prognosis - Determination of maternal serum alfa fetoprotein levels measurement - Measurement of biparietal diameter in utero
SPINA BIFIDA OCCULTA • Midline defect of the vertebral bodies without protrusion of the spinal cord or meninges • Most individuals are asymptomatic and lack of neurologic signs • In some cases patches of hair lipoma discolaration of skin dermal sinus can be seen in the midline of lower back
Neural tube defects - Spinal meningocele, myelomeningocele and myelocele • All are associated with spina bifida • Meningocele - Consists of herniation of both dura and arachnoid through a vertebral defect • Meningomyelocele • Consists of the above in addition to the spinal cord being herniated as well • Myelocele • Consists of all the above but the spinal cord is open and flat with CSF leaking on to the exposed surface • Hydrocephaly commonly occurs in association with all of the above
MENINGOCELE • Most are covered with skin and no threat to the patient • Asymptomatic children with no neurological findings may have surgery delayed • Before surgical correction plain roentgenogram,USG,MRI should be planned for determining the extent neuronal tissue involvement
MENINGOMYELOCELE • Maternal periconceptional use of folic acid supplementation reduces the incidence of neural tube defects • Lumbosacral region accounts 75%of cases • Bowel and bladder incontinence • Flaccid paralysis of the lower extremities • Absence of DTR • Lack of response to touch and pain • High incidence of lower extremity deformitties • Surgery is often done within a day of birth
Arnold Chiari Malformation (ACM)(1) • Complex deformity of the brain and cerebellum • Type 1 ectopia of cerebellar tonsils • Type 2 the most common type in neonates and usually associated with lumbar myelomeningocele Consists of lengthening of the vermis and tonsils of the cerebellum and their downward displacement through the foramen magnum in the spinal canal
Arnold Chiari Malformation (ACM)(2) - Type 3 Consists of a cervical spinal bifida, the entire cerebellum being herniated through the foramen magnum - Type 4 Cerebellar hypoplasia The malformation develops early in gestation at the age of 10 weeks
Malformations of the cerebellum • Agenesis of the cerebellum • Very uncommon • Hypoplasia • Dandy Walker malformation • Occlusion of the foramina of Lushka and Magendie of 4th ventricle early in cerebral development • Small hypoplastic cerebellum with a greatly distended 4th ventricle • Obstructive hydrocephalus and cerebellar ataxia are the clinical presentation
Ectopias and heterotopias Misplaced groups of neurons • Such as an island of gray matter in the subcortex • More common in the cerebellum than the cerebrum • Mutatons of genes directing the neurons to reach the final destination
Agyria-Lissencephaly • Total absence of gyri, • raredisordergivingtheappereance of a 3-4mnt fetalbrain, • failuretothrive, • microcephaly, • developmentaldelays, • seizures, • ocular anomalies
Pachygyria A few broad malformed gyri varying in size and number
Polymicrogyria • An increased number of gyri some of which may be abnormally small
Schizencephaly • Presence of unilateral or bilateral clefts within the cerebral hemispheres. • The borders of the cleft are surrounded by abnormal tissue • Many patients are severely mentally retarded,seizures and spastic quadriparesis
Porencephaly • Presence of cystsorcavitieswithinbraincommunicatingwiththesubarachnoidspace • Microcephaly,encephalocele,mentalretardation,spastichemiparesis-quadriparesis,opticatrophy,seizures • Holoprosencephaly • Defectivecleavage of prosencephalon • Facialanomaliesarecommon • Lobar • Singleventricle+absentfalx+fusedbasalganglia • Semilobar • Highmortalityrates • Chromosomalanomaliesandmutations
Microcephaly • Small brain usually associated with a small head • Head ofcircumference that measures more than 3SD below the mean age and sex • Primary-have no other malformations usually identified at birth familial AD • Secondary-number of etiologic agents affects the fetus in utero or an infant during periods of rapid brain growth(in the first 2 yrs of age) radiation,congenital inf,drugs meningitis/encep.,malnutrition metabolic,HIE
Megalencephaly • Proportionate enlargement of the whole brain, usually associated with the presence of a variable mental aberration - Primary - Secondary
Agenesis of corpus callosum • May be part of a complex malformation or be totally or partially absent in an otherwise normal brain • It develops between the 12 and 22 weeks of gestation • Expression from severe intellectual and neurologicalabnormalities to the asymptomatic and normally intelligent individual • Mental retardation, mild to moderate, epilepsy and cerebral palsy are common • Diagnosis can be confirmed with a CT or MRI
Hydrocephalus • Group of conditions that result from impaired circulation and absorbtion of CSF - Obstructive (noncommunicating) Resulting from the obstruction within the ventricular system - Nonobstructive (communicating) Resulting from obliteration of subarachnoid cisterns or malformation of the arachnoid villi
In a normal child 20ml/hr CSF is produced from the lateral ventricules- 3rd vent(thr foramina Monro)- 4th vent(thr aquaduct of Sylvius)- cisterns at the base of the brain(thr Luschka and Magendie foramina) convexities of cerebral hemispheres- Absorbtion(primarily by the arachnoid villi)
Accelerated rate of enlargement of the head • Anterior fontanel is wide open and bulging • Scalp veins are dilated • Eyes may deviate downward = setting sun eye sign • TREATMENT-ventriculoperitoneal shunt
HYDRANENCEPHALY • Cerebral hemispheres are absent or represented by membraneous sacs • Bilateral occlusion of the internal carotid arteries during early fetal development • İrritable child,seizures,spastic quadriparesis,no cognitive development
CRANIOSYNOSTOSIS • Premature closure of the cranial sutures • Primary-closure of one or more sutures due to abnormalities skull development • Secondary-failure of brain growth and expansion
Skull deformity-as a result of premature suture fusion • Prominent occiput • Broad forehead • Small or absent anterior fontanel
DIASTEMATOMYELIA (SPLIT SPINAL CORD MALFORMATION) • Diastematomyelia is a division of the spinal cord in to two halves by projection of a fibrocartilagionous or bony septum originating from the posterior vertebral body • It represent a disorder of neural tube fusion • The defect involves the lumbar vertebrae (L1-L3) in 50% of cases • Abnormalities of vertebral bodies • Fusion defects • Hypoplasia • Kyphoscoliosis • Spina bifida • Myelomenıngocele
Dmm CLINICAL MANIFESTATIONS • A midline abnormality of the skin in the lumbosacral region • In some cases the patients are asymplomatic • Unilateral foot abnormalities • Claw toes • Atrophy of gastrocnemius • Bilateral weakness and atrophy in lower extremities • Urinary ıncontinence • Low back pain • Loss of pain and temperature sensation
SYRINGOMYELIA • A cystic cavity within the spinal cord that may communicate with CSF pathways or remain localized and noncommunicating • Communicating syringomyelia is frequently associated with the chiari type I malformation →constriction of the central canal at the level of foramen magnum during enbriogenesis • Non communicating syringomyelia is associated with cord tumors, vascular accidents, trauma and arachnoiditis
Sm • Syringabulbia exists when the cystic cavity extends ınto the medulla • Syringomyelia rarely produces symptoms during childhood because of slow evolution
Sm • Asymmetric loss of pain and temperature sensation in the upper extremities • Muscle wasting of the hands • Absent deep tendon reflexes • Rapidly progressive scoliosis • Trophic ulcers associated with vasomotor disturbances of the hands and arms----------- loss of appreciation of pain
TETHERED CORD (TC) • During fetal development the spinal cord occupies the entire length of the vertebral column • Due to differential growth the conus medullaris in a child ultimately assumes a position at the level of L1 • Normal regression of the distal embrionic spinal cord produces a slender, threadlike filum terminale that is attached to the coccyx
Tc • TC results when a thickened ropelike filum terminale persists and anchors the conus at the below the L2 level • Neurologic signs may develop as a result of abnormal tension of spinal cord • In addition to a tight filum, sacral agenesis, intradural lipoma, myelomeningocele and dermal sinus may be associated with the tethered spinal cord syndrome
Tc CLINICAL MANIFESTATIONS • In 70% of cases inspection of the back show a midline skin lesion such as lipoma, tuft of hair, dermal sinus, portwine stain or hyperpigmentation of the skin • Signs may be evident at birth or may be delayed until adulthood • Infants may have asymmetric growth in foot or leg • Cavus deformities • Muscle wasting
Tc • The child may be delayed in walking • Toe walking • Regression of lower extremity function
Tc • The lower motor neuron signs in the legs • Abnormalities in bladder function • Recurrent urinary tract infections • Bowel incontinence • Constipation • Progressive scoliosis • Diffuse pain in the lower extremities
Tc • Plain roentgenogram = Lumbosacral bodies may show widening of the interpedicular distance hemivertabrae malformations the anterior spinal sagments • MRI = outlines the level of the conus medullaris and the filum terminale