Download
1 / 35
350 likes | 386 Views
This plan outlines Tanzania's initiative to achieve nation-wide ITN usage to combat malaria, addressing the population at risk and the burden of disease, with a focus on ITN effectiveness and strategies for public health needs.

E N D
National ITN Implementation Plan Achieving nation-wide ITN usage in the United Republic of Tanzania National Malaria Control Programme Tanzania Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Estimated Population at Risk of Malaria – Tanzanian - 2000 • Population • Total 33.8 million (100%) • At risk of malaria 31.6 million (93.7%) • Population at risk where transmission lasts: • >6 months (stable, perennial) 14.1 m (42%) • 4-6 months (stable, seasonal) 11.3 m (33%) • 1-3 months ( strongly seasonal/epidemic) 2.6 m (8%) • <1 month (epidemic/no malaria in avg.Year) 5.8m (17%) Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Tanzania’s Burden of Disease Malaria: • Estimated 16 million malaria cases per year • Consumes 119 million US $ per year (3.4%GDP) • Most deaths in under-five children and pregnant women • Under 5 year child deaths estimated at 161,000 (per 1000 live births) per year of which 39,000 due to malaria Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
ITN Effectiveness • Results of large scale ITN trials in Africa: • Overall 20% reduction in ‘all cause’ child mortality • Overall 50% reduction in malarial illness • Effective at all levels of transmission • 5.6 deaths averted per 1000 children per year • Despite < 70% compliance Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
ITN Effectiveness • KINET evidence – for treated net users: • Childhood (1 month – 4 years)protective efficacy of 27% • 63% less parasitaemia • 63% less anaemia • Children generally healthier and grow better • Protected pregnant women 12% less anaemia • Despite low re-treatment rates in an area of perennial transmission with very high biting rates • For children under 5 alone this could translate into more than 30,000 deaths averted per year in Tanzania Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Why ITNs in Tanzania ? • High need • Strong research-based effectiveness evidence • Cost-effectiveness advantage • Public sector becoming more responsive • Energetic private sector • Expanding district level involvement • NGOs engaged and willing • Renewed commitment from donor partners • Evidence of increased household expenditure Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Where do we want to go ? High utilization of ITNs through more equitable access What does this mean for Tanzania ? • Present coverage – • <50% of children sleep under any net • Coverage of ITNs is greater, in project areas (up to 30%) when compared to non project areas • Areas with ITN projects, 13 – 28 % ITN coverage • Overall net usage 80% in some towns, 50% in rural areas Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Targets By 2007: at least 60 % of children under 5 years of age and pregnant women will be sleeping under an appropriately treated mosquito net Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
How to meet Public Health Need? • Donors and Government unable to meet costs of project type social marketing • Commercial sector is already successfully marketing Nets and treatment kits • Local commercial distribution is more efficient than projects (mark-up $2-$4) • Must use public funds in the most effective way • So - Need to target resources to those most at risk without reducing commercial sales Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Public Sector ITN Distribution ? • Attractive opportunity – promote and sell nets at clinics • Revolving funds at clinic / district level hard to administer – large losses reported • Temptation to take excess profit so cost not reduced • Public Health facilities is not the best option for delivery of ITNs Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Commercial Sector involvement • Sales grown to more than 1.5 million per year through existing commercial networks – mainly urban • Combined production of the three net manufacturing companies – 4 million nets per annum • Key partnerships with insecticide producers – kit price now $ 0.35 • Retail price of nets: $2.6 – $3.6 Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Enabling Factors • Establishment of ITN Multisectoral Task Force • Strong local research base • Strong and growing manufacturing sector • Donors prepared to invest and encourage manufacturers through demand creation • Dynamic, committed, social marketing team • Committed individuals supporting development of plan – NMCP, MoH, Researchers, Private sector, NGOs, donors. Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Enabling Factors • Removal of taxes and tariffs on both nets insecticides Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Challenges • Advocacy – reaching a critical mass • Sustainability of the momentum which has substantial donor support • Concurrent activity when human resources are over stretched • Net use in rural areas is still strongly seasonal, yet malaria transmission is all year round Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Challenges • Reaching those who truly may not be able to afford a net • Balancing public health gain and private cost Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
So The way forward Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Strategic Approach • Demand creation - Government / Donor funded and contracted out • Production, distribution, sales - Private sector • Regulatory coordination - Government (NMCP) and regulatory instruments of the govt. • Monitoring and Evaluation / Research - Government(NMCP)coordinated / contracted out / research partners • ITN Steering Committee - Multi-stakeholder • Coordination and Management –NMCP based Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
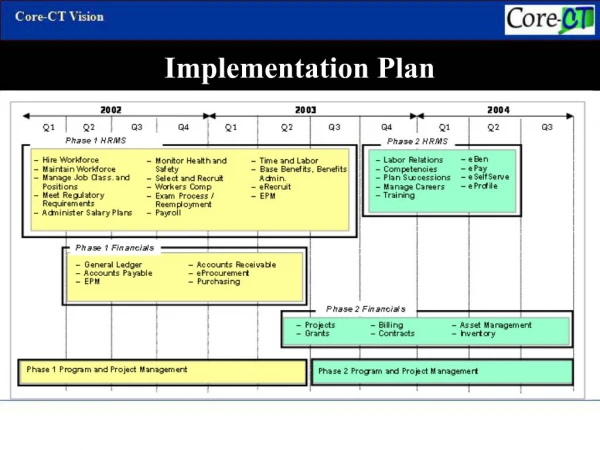
Implementation Plan • ITN Steering Committee formed from Task Force • Responsible to MoH • CMO and NMCP Manager on Steering Committee • Implementation Team a ‘cell’ within NMCP • Implementation Team Leader reports to Steering Committee Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Implementation Team Role • Advocacy / Negotiation • Management of process • Demand creation co-ordination / contracting • Research co-ordination / contracting • Management of Voucher scheme • Regulatory / Revenue lobbying • Financial management • Technical advice / support to Districts Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Public / Private partnership • Implementation Team role to: • Co-ordinate • Facilitate • Negotiate • Broker agreement Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Role of Social Marketing • Concentrates on commercial alliances to increase net availability in rural areas • Promotes a ‘national brand’ of Insecticide (Ngao) for a variety of different net treatments – consumer confidence and recognition, while encouraging competition to reduce cost. Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Evolving Partner Contributions START Production PUBLIC SECTOR PRIVATE Distribution Consumer information Distribution Demand Creation Create enabling environment Household / community demand creation Equity & Vulnerable groups Distribution Research Partners Donor Partners NGOs Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Desired Framework for Partners PUBLIC SECTOR PRIVATE SECTOR National generic demand creation Consumer information Brand specific demand creation National co-ordination Consumer protection - regulatory issues Supply & Sales Demand Creation Product development Create enabling environment Household / community demand creation Distribution Distribution Equity & Vulnerable groups DONOR PARTNERS RESEARCH PARTNERS NGOs Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Core activities of Social Marketing within evolution of ITN Implementation Plan 70% 2007 Market mature, NMCP subsumes role of Implementation Team. ITN projects, except equity based, phased out. Evaluation, monitoring and essential promotion MoH funded. Social Marketing (promotion) 2005 50% Market Maturing Implementation Team Operational: Advocacy, technical support, Contracting of activities to Private sector. KINET and other equity based projects Social Marketing (promotion and distribution) Coverage 2002 10% Implementation team funded Market Forming Social Marketing (promotion, distribution and advocacy) 2000 Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
The availability of Nets and Insecticides in the country • Maximum choice of ITN commodities • Facilitated co-operation between TPRI / TBS and net/insecticide manufacturers • Nets bundled with Insecticide • Agreement reached that all nets sold will be with insecticide (c.f. iodised salt) • Insecticide kits Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
GFATM proposal for malaria • Equitable targeting to highest risk groups • Pregnant women and infants • Voucher system • linked to uptake of essential health interventions • antenatal clinic attendance, EPI uptake • high value to encourage uptake • MCH staff distribute, Banks cash voucher Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Vouchers • benefits • encourages private sector sales and rural penetration • will not destabilise market • readily identifiable qualification (pregnancy) • less administration for health staff • could pull antenatal and EPI coverage up Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Vouchers • risks • Fraud, high value high risk • Retailer refusal to honour voucher • Banks refusal to co-operate • Retailers don’t get money • Who uses the ITN in the home ? Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Subsidy – Research Gaps • Market research - who truly still needs subsidy • Commercial sector slow to engage in the process (voucher scheme) • Extent of Black market (leakage of voucher) • Definition of criteria for access ? • Monitoring and Control systems ? • Audit • Cost ? Risks ? Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Accelerated Access • Requires • Massive effort • Significant extra resources • GFATM approval • Bilateral support is time limited • New ways of working • Contracting out • Private sector skills public sector • Stakeholder co-ordination Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
District Activities • Persistent behaviour change requires: • Integrated district / community activities that encourage adoption of new ideas Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Community empowerment Changing behaviour Empowering women Income generation Fair pricing BUT - Who makes the choices ? Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
Consumers • Prioritising health needs – knowledge based • Local availability of low cost ITN supplies • Economic gains from reduced malaria burden • Increased human capital • Maintain long term view Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002
AHSANTE SANA Tanzania ITN Implementation Plan – RBM/IMCI Harare 2002