Download
1 / 80
820 likes | 890 Views
BENIGN PROSTATE HYPERPLASIA. Assistant Professor Hakan KOYUNCU Yeditepe University Medical Faculty Urology Department. BPH GLANDULA FIBROMUSCULAR STROMA is the hyperplasia of these components of the prostate and it is not malignant. Hystological existence of BPH

E N D
BENIGN PROSTATE HYPERPLASIA Assistant Professor Hakan KOYUNCU Yeditepe University Medical Faculty Urology Department
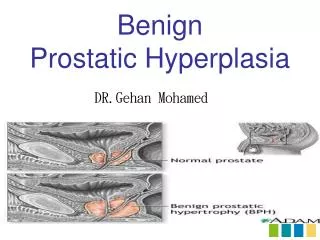
BPH GLANDULA FIBROMUSCULAR STROMA is the hyperplasia of these components of the prostate and it is not malignant.
Hystological existence of BPH • Around fourties % 8 • 51 - 60 years old % 40 • 61 - 70 years old % 60 • Above the age of 80 % 90
BPH Prevalence-1 • 40–49 yearsold % 13.8 • 50–59 yearsold % 24 • 60–69 yearsold % 43 • About % 30 of malepopulation is having a surgicaloperationbecause of thelongerlifetimes.
BPH Prevalence-2 • Hystologic BPH is not seen before the age of 30. • The incidence increases by the age and it reaches the maximum level at 9th decade. • Palpable hyperplasia of the prostate is seen in %20 of the patients aged at 60 and in %43 of the patients at the age 80. • Prostate hyperplasia is not always correlated with the clinical symptoms and signs.
Histology of the prostate • Prostate consists of three distinct zones: a central zone, transitional zone and peripheral zone. The TZ is the site of development of BPH. • According to the anatomy of the ducts; the prostate is composed of approximately 30-50 glandular structures which are spread out into a matrix of fibromuscular stroma. • The glands open to the prostatic urethra from both sides of veru montanum, by 16-32 excretuar channels. • Approximate weight of the prostate in adults is 18-20 gr.
Epithelial cells consist of 4 main cell group. • Prostatic aciner and secretory cells • Basal cells • Transitional cells • Endocrin-paracrin cells
Bph is a clinical terminology. • There is a lower urinary system disfunction composed of the changes secondary to obstruction or the age. The changes are on the stability and the contractility of the bladder because of the infravesical obstruction dependant to prostate hyperplasia.
Etiology • Histopathologically, BPH is characterised by the increase of the epithelial and stromal cells on the periuretral side of the prostate. • The molecular mechanism of this hyperplastic formation is not clear but it is concluded that there are a lot of factors effecting the formation of BPH.
Etiology Aging Functional Testis
Factors on etiology-1 • Aging -Testesteron (leydig cells) decrease. -SHBG increases, serum testesteron levels decrease. -Intraprostatic DHT and androgen reseptor levels increase. -Free estrogen / free testesteron level increase.
Factors on etiology-2 • Role of androgens They are the major trigger in the formation of BPH. 5α reductase Testosteron Dihydrotestosteron (DHT) • DHT is the major intraprostatic testosteron and its’ affinity to androgen receptors are more than testosterons’ .
Factors on etiology-3 • Role of estrogens • It is concluded that estrogens have a synergistic effect together with androgens. • Increases the number of androgenic receptors (?) • Increases the level of intraprostatic DHT by increasing the transformation of testosteron to DHT.
Factors on etiology-4 • Prostate evolution in embrionic life occurs by the stromal-epithelial interaction under the support of androgens. • Mitogenic effect of the androgens take place only if there are stromal cells around.
Factors on etiology-5 • 5-alpha-reductase are mostly in stroma, also androgen dependant epithelial growth is only possible by the existence of stromal components in tissue cultures. • These information support the idea of stroma-epithelium interaction.
There are studies showing that epithelial growth effect of stromal cells take place by the mediation of paracrin mechanism, growth factors and proto-oncogens.
Growth Factors effective on BPH • Keratinocyte growth factor (KGF) • Epidermal growth factor (EGF) • Insulin-like growth factor (IGF-1/2) • Fibroblast growth factor (FGF) • Transforming growth factor (TGF)
Result • BPH appears as the reactivation of the embrionic growth potential in stroma, by the effect of age-dependant hormonal changes and peptid-like growth factors.
Factors on etiology-6 • Genetic predisposition BPH Familial Sporadic 1- 3 or more people who has 1-Prostate volume BPH in family history (Approx. 55.5) 2- Starts at early age ( There is a hereditary effect in % 50 of the people who had a prostate operation before the age 60) 3- Big prostate volume (Approx. 82.7)
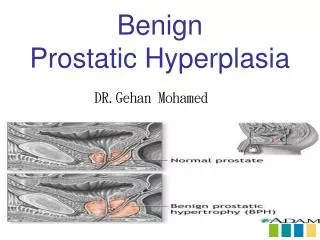
Patophysiology of Obstruction • Consists of 3 stages • Anatomic obstruction • Primary patophysiologic obstruction (High pressure in the proximal of the obstruction) • Secondary patophysiologic obstruction (Retantion - Infection – Hydronephrosis)
Changes in the uretra in BPH Morphologic deformity ***(Deformation) Longer in length ***(Elongation) Changing the position ***(Deviation)
Answer of the Bladder to BPH • Starting period • Compensatory stage • Decompensatory stage
Lesions in Compensatory stage • Trabeculation • Cellula • Diverticula
Lesions in Decompensatory stage • The scar tissue replaces the muscle. • The ejaculation function decreases progressively. • Compliance decreases. • The pressure increases. • As a result: Detrusor instability
Upper urinary system in future time • Bilateral ureterectasia • Ureterohydronephrosis • Result: Chronic renal failure
BPH-Clinical Features In time, prostate volume can increase, symptoms get worse, urinary flow rate decrease, acute urinary retention can form, and in some patients surgery can be a necessity. !!!!BPH IS MOSTLY A PROGRESSİVE DISEASE!
Complications • Acute urinary retantion • Urinary system infection • Bladder stone • Bladder injury • Renal failure • Hematuria
Diagnose • Medical history • Symptom Score • Physical examination • DRE and limited neurological examination • Diary of miction • Urine analysis • Creatinine • PSA ?? • Urinary flow rate • PMR
Symptoms in BPH Irritative • Nokturia • Pollakiuria • Disuria • Urgency Obstructive • Poor urine flow • Delay and difficulty in starting the miction • Postmictional dripping • Feel of not-emptying after miction • Urinary retantion • Overflow incontinence
Symptom Scores in BPH • Boyarsky • AUA • I-PSS • Turkish Symptom Score adapted from I-PSS
IPSS • Total symptom score differs between 0-35 and grades the mictional disfunction • 0-7 mild • 8-19 moderate • 20-35 severe
Laboratory and Radiologic Evaluation • Urine analysis, creatinine • PSA • Ultrasonography Urinary Transrectal • IVP • Uroflowmetry
Uriner analysis • Recommended because of that it shows the hematuria and urinary infection
Creatinine • It is established that higher creatinine levels increase the post-operative complications • Creatinine examination is recommended
PSA • Prostat spesific antigen (PSA) is a glicoproteine based protease which is secreted from the prostate epithelium cells. • BPH causes a mild/moderate increase in PSA. • Normal PSA level? 4? 2.5?
PSA • Between 50-70 years old, every year PSA ve DRE is recommended. • PSA ve DRM starts at 40 years old for the ones who has family history
USG or IVP (for who?) • Hematuria • Urinary stone history • Urinary infection history • Urogenital surgery history • Failure in renal functions
IVP Prostatic indentation - Fish-hook like presentation - Bladder stone - İncrease in trabeculation, cellulas and diverticulas. - Determining residual urine in post-voiding graphy.