Download
1 / 50
640 likes | 1.58k Views
Catecholamines. Author: Eva Klapková. The catecholamines (epinephrine, norepinephrine and dopamine) and serotonin belong to the group of biogenic amines. They act as neuromodulators in the centra l nervous syst em and as hormones in the blood circulation.

E N D
Catecholamines Author: Eva Klapková
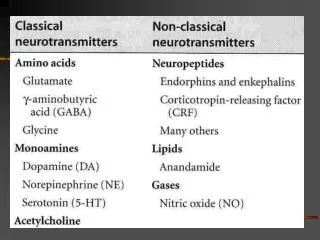
The catecholamines (epinephrine, norepinephrine and dopamine) and serotonin belong to the group of biogenic amines. They act as neuromodulators in the central nervoussystem and as hormones in the blood circulation.
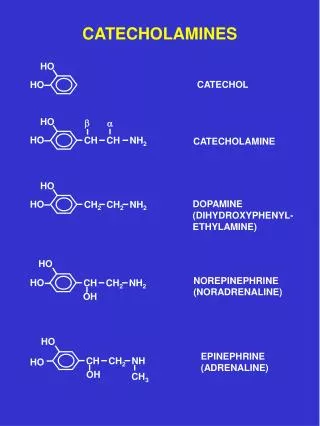
Physiologically relevant catecholamines are epinephrine, norepinephrine and dopamine. • Epinephrine (E) has been considered a classic example of a hormone and norepinephrine (NE) a neurotransmitter but both function reciprocally. • E is produced primarily by the chromaffincellsoftheadrenalmedulla and NE by the sympathetic neurons but they both have similar structures and biological actions.
Pathways of catecholamine biosynthesis withinthe CNS, sympathetic neurons and chromaffin tissue appear to be identical. The number of steps in each pathway depends on the product, DA, NE, or E. • Catecholamines derive from theaminoacidtyrosine. • Tyrosine is created from phenylalanineandisalsoingested directly from dietary protein .
Tyrosine is transported into the cell where it is converted to dihydroxyphenylalanine (DOPA) by tyrosine hydroxylase. • Conversion of tyrosine to E involves four steps: 1) hydroxylation of the phenolic ring, 2) side chain decarboxylation, 3) side-chain hydroxylation, 4) N-methylation.
Conversion of tyrosine to DOPA is the rate limiting step in catecholamine biosynthesis. Activity of the enzyme is controlled by end-product inhibition by cytoplasmiccatecholamines. • Chronic stimulation of catecholamine synthesis and secretion leads to elevation of cellular tyrosine hydroxylase levels. • DOPA is then decarboxylated to dopamine (DA) by DOPA decarboxylase, a nonspecific decarboxylase found in many tissues.
DA is then hydroxylated by dopamine--hydroxylase (DBH). In dopaminergic neurons DA is the final step, in noradrenergic neurons DA is converted to NE within the chromaffin granule. • The NE produced is converted to E by phenylethanolamine-N-methyltransferase (PNMT) outside the granule. This enzyme is only found in cells that synthesize E (adrenal chromaffin tissue).
Biosynthesis of catecholamines
In species where the chromaffin tissue is separated from the adrenal steroidogenic tissue, NE is the main product. In those species where the chromaffin tissue is contiguous with the steroidogenic tissue, however, E is predominant (humans).
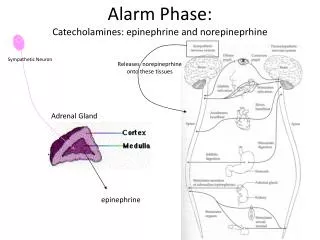
Storage and Release • Catecholamines (E or NE) are contained in granules wherein they are complexed with ATP, and a specific protein, chromogranin and DBH. E is synthesized and stored in the granule but NE is made outside the granule, then stored here. E and NE are contained in different cells. • Secretory vesicles are released through a stimulus-secretion coupling requiring Ca++. All the contents of the granules are released during vesicular exocytosis.
The loss of DBH from the chromaffin cells when the content of the granule has been exhausted provides evidence for the fact that an interval is required to produce E again in high levels. • Once E is secreted into the bloodstream, it affects a receptors on hepatocytes to increase blood glucose and it interacts with a receptors on vascular smooth muscle cells to cause contraction and increase blood pressure.
Metabolism of Catecholamines • Catecholamines are catabolized by 2 enzymes, catecholamine-O-methyltransferase (COMT) and monoamine oxidase (MOA). • NE and E are metabolized extracellulary by COMT to normetanephrine and metanephrine, respectively. • COMT is localized in the cytosol of sympathetic effector cells and is also found extracellularly in close proximity to adrenoceptors of autonomic effectors. Increased activity of COMT in response to catecholamines provides a homeostatic mechanism for rapid removal of catecholamines from the circulation and synaptic cleft.
MAO is found in the surface of the outer membrane of the mitochondria where it limits the accumulation of catecholaminesin the cytoplasm. • Sequential action of COMT and MAO leads to the main metabolite excreted in the urine, 3-methoxy-4-hydroxymandelic acid (vanillylmandelic acid, VMA).
Metabolism COMT – catechol-o-methyltransferase MAO – monoaminooxidase
Phenylalanine 3-methoxytyramin HOMOVANILIC ACID Tyrosine DOPA DOPAMIN 3,4-dihydroxyphenyl acetate Adrenaline Noradrenaline Metanephrine Normetanephrine dihydroxymandel aldehyd (DHM-ald) 3-methoxy- -4-hydroxy-mandel Dihydroxymandelic acid Dihydroxy- aldehyd phenylglykol Vanillylmandelic acid (VMA)
Most of the NE released from the sympathetic neuron is taken back up into the neuron where it is either transported into secretory vesicles or destroyed by MAO. • The NE accumulated within the synaptic cleft feeds back to an adrenergic receptors within the presynaptic membrane and this stimulates uptake and inhibits further synthesis of NE.
Function Maintain homeostasis – acute or chronic stress Neurotransmiters CNS Neurohormonal transmiters of adrenal medulla
The abnormal production or secretion of catecholamines is typical in neuroendocrine tumors (pheochromocytoma, neuroblastoma, paragangliomas) The determination of levels of catecholamines a their metabolites enables an early detection of tumors and monitoring of treatment. Common radiodiagnostic examinations (sono, CT, NMR, PET) serve for confirmation of laboratory tests and localization of tumors.
Pheochromocytoma • Neuroendocrine tumor secretes high amounts of catecholamines • Usually noncancerous (benign) tumor that develops in the core of an adrenal gland • About 10% of adrenal cases are bilateral (suggesting hereditary disease) • About 10% of adrenal cases occur in children (also suggesting hereditary disease) • About 15% are extra-adrenal (located in any orthosympathetic tissue): of these 9% are in the abdomen and 1% are located elsewhere. Some extra-adrenal pheochromocytomas are probably actually paragangliomas, but the distinction is only possible after surgical resection.
About 11.1% of adrenal cases are malignant, but this rises to 30% for extra-adrenal cases • About 26% are hereditary (earlier opinion had 10%) • About 3% recur after being resected • About 14% of affected individuals do not have arterial hypertension • Up to 25 % of pheochromocytomas may be familial (multiple endocrine neoplasia, type II (MEN II); von Hippel-Lindau disease; familial paraganglioma; or neurofibromatosis 1 (NF1))
excessivecatecholaminesecretion(primarilynorepinephrine) • common sign ishighbloodpressure • most people has persistenthighbloodpressure • sometimeswithfluctuation (intermittentreleaseofhormones) • signsandsymptomsmayinclude: high blood pressure, rapidheart rate, forceful heartbeat, profound sweating, abdominal pain, sudden-onset headaches — usually severe — of varying duration, anxiety, feeling of extreme fright, pale skin, weight loss • if the diagnosis of a pheochromocytoma is overlooked, the consequences can be disastrous, even fatal (myocardial infarction,dilated cardiomyopathy, and pulmonary edema,cerebralinfarction) • earlydiagnosis – measuring catecholamines and metanephrines in plasma (blood) or through a 24-hour urine collection
the production of E and NE is not specific only for pheochromocytoma • silent pheochromocytoma – sporadic releasing of catecholamines • free metanephrines are produced continuously within pheochromocytoma tumor cells and independently of catecholamine release– great importance for detection of pheochromocytoma Development of new procedures for measurement of plasma free metanephrines
Treatment: • surgical resection of the tumor - the treatment of first choice • (open laparotomy or else laparoscopy) • prior treatment with the non-specific and irreversible alpha adrenoceptor blocker
interpretation of results X false positive renovascular hypertension, hypotension, hypovolemia, hypoglycemia, stress, sepsis, dumping syndrom, sleep apnea different preanalytics procedures
diet: bananas, oranges, grapefruits, tomatoes, nuts, cheese, chocolate, cacao, tee. coffee, alcohol, vanilla, foods with vanillin medikaments: betablockers triamteren alfablockers methyldopa antihypertensives mandelamin inhibitors MAO disulfiram antibiotics benzodiazepins chinin, chinidin solatol chlorpromazin labetalol
Advantage of plasma free metanephrines determination: blood collection– few minutes calming, vein cannulation is necessary results – not affected by food (caffeine) drugs (tricyclic antidepressants, betablockers) Disadvantage of plasma catecholamines determination: blood collection– long-term bed rest (more than 12 hours) results – can be affected by various food (diet necessary), drugs, and physical and psychological stress
Neuroblastoma NB is the most common extracranial solid cancer in childhood (> 50% in children < 2 years) Neuroendocrine tumor arising from any neural crest element of the sympathetic nervous system Location: abdomen (70% thereof ½ adrenal), 20 % in the chest, in the bones, pressing on the spinal cord Symptoms: diarrhea, ataxia, swollen belly, constipation neurological symptoms (weakness, inability to stand, crawl or walk, limping, pain)
Laboratory tests Basic: blood counts (50-60 % anemia), FW; Fe, ALT, AST, GMT, ALP, urea, creatinine, urine+sediment vanillylmandelic acid in urine Special biochemical tests: homovanillic acid (end metabolite of dopamine) L-DOPA (3,4-dihydroxypheenylalanine – precurzor of dopamine), VMA/HVA: better prognosis; noradrenaline, dopamin, metanephrine, normetanephrine, dihydroxyphenylacetate (DOPAC)
Diagnostic schema for pheochromocytoma determination of free metanephrines in plasma (ng/l) Both metabolites are in reference range (<112 NMN, <61 MN) Unlikely tumor One or both metabolites are elevated Slightly elevated(<400 NMR, <236 MN) Significantly elevated(>400 NMR, >236 MN) possible tumor highly probable tumor Check the elimination of influence of diet or therapy Determination of A, NA, calculation of ratio MN/A and NMN/NA Increase of ratio NMN/NA >0,52 or MN/A >4,2 highly probable tumor Normalization of both metabolites Unlikely tumor >>NMN či MN ratio but <cut-off Clonidine suppression test normal, unlikely tumor pathological, highly probable tumor Other clinical and laboratory observation Localization of tumor (CT, NMR, PET)
Clonidine suppression test • 0.3 mg of clonidine applied • Samples taken before clonidine application, and 3 hours after • Doctor’s supervision necessary • Estimation of MN, NMN, E, NE Positive • Decrease NMN < 40 %, NE < 50% • No decrease in plasma levels
Screening following Diagnostic schema for pheochromocytoma Patient, female, born 1949 Metanephrine< 30.0 (0-61) ng/l Normetanephrine< 60,0 (0-112) ng/l Index MN/E 0.6 (0-4.2) Index NMN/NE 0.17 (0-0.52) Epinephrine 50.4 (0-84) pg/ml Norepinephrine 360.9 (250-420) pg/ml The values do not indicate presence of pheochromocytoma
Patient, male, born 1940 Metanephrine 30.3 (0-61) ng/l Normetanephrine< 60.0 (0-112) ng/l Index MN/E 0.57 (0-4,2) Index NMN/NE 0.10 (0-0,52) Epinephrine 53.4 (0-84) pg/ml Norepinephrine575.4 (250-420) pg/ml The values do not indicate presence of pheochromocytoma (secondary stress)
Patient, female, born 1945 Metanephrine41.8 (0-61) ng/l Normetanephrine 72.1 (0-112) ng/l Index MN/E 0.38 (0-4,2) Index NMN/NE 0.05 (0-0,52) Epinephrine 109.3 (0-84) pg/ml Norepinephrine1342.6 (250-420) pg/ml The values do not indicate presence of pheochromocytoma (secondary stress)
Patient, female, born 1942, 10 years ago underwent surgery adenoma of adrenal gland Metanephrine< 30.0 (0-61) ng/l Normetanephrine113.7 (0-112) ng/l Index MN/E 0.26 (0-4,2) Index NMN/NE 0.14 (0-0,52) Epinephrine 115.7 (0-84) pg/ml Norepinephrine 803.4 (250-420) pg/ml Increasedlevel of normetanephrine, consider clonidine test. Increasedlevels of catecholaminescan be caused by secondary stress CT examination did not prove presence ofpheochromocytoma
Patient, male, born 1953 Metanephrine1154.2 (0-61) ng/l Normetanephrine2539.3 (0-112) ng/l Index MN/E 33.46 (0-4,2) Index NMN/NE 10.88 (0-0,52) Epinephrine 34.5 (0-84) pg/ml Norepinephrine 233.4 (250-420) pg/ml Catecholamines normal, free nephrines increased, indexes increased Suspect pheochromocytoma of adrenal localization.
Case study - hypertension Male – 50 years, regular check, every two years 185 cm, 90 kg, BMI = 26.3 BP 150/100, P 96/min, no pathological changes, EKG normal Recom.: urine + sediment, Retinal examination, FW, KO, liver enzymes, creatinine, uric acid, NA, K, Cl, Ca, glycemia, lipida, TSH, fT4, PSA Therapy: Metropolol twice daily, slim Check 3.11.: BP 170/105, P 90 min, sweating 1-2 weekly Check 18.11.: BP 150/95, P = 80/min, no sweating, pressure in liver areas Therapy: Metropolol, Amlodipin in morning Check 30.11.: BP 135/85, P = 84/min, check in a month Check 15.12. BP 150/95, P = 90/min, twice increased strong sweating without accompanying strain, booked Holter’s monitor Check 15.2. Variable BP up to 190/120, abdomen USG – susp. enlarged right adrenal gland VMA in urine , week leukocytosis, CT – hypertrophy of right adrenal gland
Early pheochromocytoma detection Minimal symptoms Usage of beta-blockers worsened hypertension
Diagnosis ofboth-sidepheochromocytoma 28 year old, female, medullar carcinoma of thyroid gland - syndrome MEN 2b During 8th year of primary schools diagnosed enlarged thyroid, appliedthyreoglobulin In 1991 sonography of thyroid, diagnosed pathology, surgery subtotal strumectomy – histologically proved medullar thyroid carcinoma In 1992 found calcified remnant of thyroid gland and nodus in the scar, underwent surgery From 1996 fluctuating blood pressure, increase VMA in urine and increased level of calcitonine (negation of heat waves, headache, sweating, tired) 1998 CT of adrenal gland negative (suspected pheochromocytoma) 123I scintigraphy repeatedly rejected, neck sonography without marks of relapce 2003 CT of adrenal gland and 123I scintigraphy – proved both-side pheochromocytoma Calcitonin (1996) – 296.7 pg/ml, increased up to 1125.5 pg/ml VMA (1997) – 42.8 mol, increased up to 118.6 mol (normal 5-35 mol)
Neuroblastoma Boy 2.5 months, SVD, 4 kg, 51 cm, well thriving, no illness 9th week after birth enlarged abdomen Found hepatosplenomegalia – transferred to FH Motol, suspected metabolic syndrome Proved hepatosplenomegalia, developing deposit in liver, and clusters of unripe cells in bone marrow – suspected neuroblastoma Laboratory exam: HVA 298 mmol/mol creatinine VMA 246 mmol/mol creatinine DOPAC 1.2 mmol/mol creatinine 5-HIAA 1,4 mmol/mol creatinine AST 2.95 ukat/l GMT 3.37 ukat/l LD 14.0 ukat/l Total protein 34.9 g/l Albumin 26.1 g/l IgG 1.8 g/l
Started antitumor therapy, 5 seriesin 4 months After 3seriesdecreased hepatomegaliaand primary tumor After 5thseriesliver size decreased, andgradual regresionof primary tumor Laboratory exam : HVA 14.2 mmol/mol creatinine VMA 6.8 mmol/mol creatinine DOPAC 0.9 mmol/mol creatinine AST 0.75 ukat/l LD 5.8 ukat/l Bone marrow and blood exams normal Total remission.
2.5 years old, girl, SVD 4.2 kg, 53 cm, well thriving, no illness After fall from staircase (no consequent problems) tired, feeling cold, no appetite, insomnia Then occurrence of veins on upper eyelids, next day hematoma Ophthalmology check revealed retinopathy Observed hepatomegaly, palpable resistance in right part of abdomen Sono – observed resistance in the area of right adrenal gland Check: LD 180.4 ukat/l VMA 10.9 mmol/mol creatinine (0.4-4.0) HVA 97 mmol/mol creatinine (1.05-2.0) DOPAC 15.2 mmol/mol creatinine (1.0-1.3) 5-HIAA 9.6 mmol/mol creatinine (2.0-2.6) Head CT: metastatic process in right orbit Abdomen CT: neuroblastoma of right adrenal gland, blood perfusion Skeleton RTG: diffuse, thinner skeleton
Carcinoid Tumours producing mainly serotonin, and its metabolites, however, other biol. active compounds (chromogranin A, histamine, insulin, glucagon, …) were observed Variable clinical symptoms – called carcinoid syndrome (10-30 %) flush syndrome, skin problems, diarrhoea, cardiatic symptoms, abdominal pain bronchospasma, hypotension Diagnosis - 5-HIAA estimation
Patient, female, born 1963 For half a year observed - intermitent diarrhoea CT of pancreas / negative Pancoloscopy – diffused distinct vein depiction, no pathology After 2 month UC of epigastrium – non/characteristic changes on the border of body and pancreatic cauda Check food allergies Observed allergy to apples – result: focal pancreatitis and food allergy After 2 months again UC of epigastrium, persistent diarrhoea, unclear observetion CT of pancreas – focal pancreatitis with partial thrombosis, unobstructive in v. portea Hospitalization, started anticoagulation treatment, MRI, UC – Thrombus size 2.6 cm Laboratory check – everything in reference (amylases, KO, urine, CA 19-9, CEA, 5-HIAA) After treatment reduction of reported health problems size of thrombus increased to 5 cm In one year apparent dilated veins medial from spleen, splenomagaly, thrombus as a soft tissue deposit
Patient transferred to FH Motol with diagnosis of portal hypertension with pre-a intrahepatal blockade, unclear observation in pancreas Per-surgery diagnosis – pancreatic adenocarcinoma with metastasis in lymph node tumourous thrombus in v.portale – final diagnosis> carcinoid Patient with unusual case of thrombosis on lienal and portal vein with complicated and long lasting search form tumour ethology (biochemical check all the time negative)
Patient, female, born 1949 Admitted fro hospitalization du to diarrhoea, loud systolic mourmour, liver 3 cm over rib arc, facial teleangiectasias, other observations normal Subjective symptoms: worsening diarrhoea, seizures of dyspnoea , weight loss Gastroscopy and colonoscopy negative Repeated liver UC – deposit in liver, non metastatic Admitted to GM after UC, and kardioechographic check diagnosed - suspection of generalized carcinoid Laboratory: 5-HIAA 810 umol/day (47 umol/day) and Serotonin 3.17 umol/day (1.4 umol/day) Total protein 56 g/l albumin 34 g/l Liver enzymes increase
Patient, female, born 1957 Transferred to oncology withdiagnosis of metastatic liver damage CT – observed neuroendocrinouscarcinoid, primary tumour in colon ascendens, metastasis inliver, in medialsternal manubrium, in medial hypogastrium, radiotherapy Laboratory: 11.5.2012 CEA, CA 19-9, CA 125, AFP normal GGT 1.51 ukat/l (0.14-0.68) VMA 1.0 mmol/mol crea (1.0-2.0) 5-HIAA 85.7mmol/mol crea (1.0-1.5) HVA 3.3 mmol/mol crea (0.6-2.5) 8.10.2012 GGT 8.47 ukat/l ALT 1.02 ALP 3.95 VMA 2.0 mmol/mol crea 5-HIAA 131.8 HVA 5.2
18.12.2012 GGT 5.56 ukat/l ALP 2.34 ukat/l AST 1.90 ALT 2.71 LD 4.16 VMA 1.5 mmol/mol crea 5-HIAA 146.4 HVA 2.0 13.3.2013 VMA 1.3 5-HIAA 135.1 HVA 2.4 7.6.2013 VAM 1.7 5-HIAA 151.2 HVA 3.4 15.1.2014 GGT 9.71 ukat/l ALP 6.47 VMA 1.4 mmol/mol crea HVA 1.7 5-HIAA 187.1



![Catecholamines (dopamine [DA], norepinephrine [NE], epinephrine [EPI])](https://cdn2.slideserve.com/3865027/catecholamines-dopamine-da-norepinephrine-ne-epinephrine-epi-dt.jpg)