Download
1 / 82
860 likes | 1.49k Views
BENIGN PROSTATIC HYPERPLASIA. Assoc . Prof .Hakan KOYUNCU Yeditepe University Medical Faculty Urology. BPH is the benign enlargement of prostate due to glandular & stromal hyperplasia. Presence of BPH 4 th decade % 8 51 - 60 years % 40

E N D
BENIGN PROSTATIC HYPERPLASIA Assoc.Prof.Hakan KOYUNCU Yeditepe UniversityMedical Faculty Urology
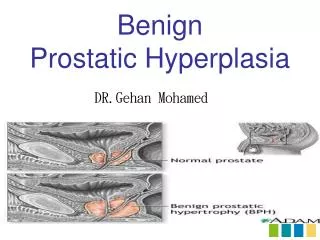
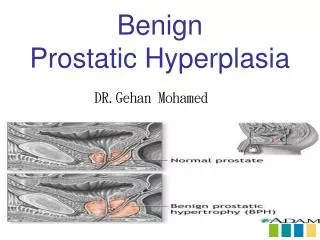
BPHis the benign enlargement of prostate due to glandular& stromal hyperplasia
Presence of BPH • 4th decade % 8 • 51 - 60 years % 40 • 61 - 70 years % 60 • + 80 years% 90
BPH Prevelance-1 • 40–49 age group % 13.8 • 50–59 age group % 24 • 60–69 age group % 43 As life expectancy rises, 30% BPH is being operated on
BPH Prevelance-2 • Hystologic BPH is seen after the 3rd decade • Incidence increases with age, peaks at 9th decade • Palpableprostate enlargement in 20% of 60 year olds and 43% of 80 year olds • Prostate enlargment does not always present symptoms
Hystologic structure • Composed of fibromuscular stroma,consists of 30 - 50 tubulo-alveoler glands • Glands open to Verumontanum via 16 - 32 excretory channels to prostatic urethra • Average weight is around 18 -20 gr
Epithelial cells consist of 4 main types: • Prostatik acineror secretorycells • Basal cells • Transitional cells • Endocrine-paracrine cells
Prostat hiperplasiais the benign growth of prostate due to changes in glandular and/or fibromuscular elements • All cell types may increase, mostly SECRETORY HYPERPLASIA is observed
The enlarged prostate causes infravesical obstructions, which affects bladder stability and contractility. • Changes can be due to above mentioned obstructions or due to the age of the patient • BPH is a lower urinary tract dysfunction
ETIOLOGY • Histopathologically characterized by increased number of epithelial and stromal cells in periurethral prostate • The mechanism is still unknown but it is known that many factors play a role in BPH
ETIOLOGY Aging Having functional testis
ETIOLOGICAL FACTORS • Aging -Testosteron (leydig cells)production↓ - Sex hormone binding proteins↑serum testosteron level ↓. -Intraprostatic DHT and androgen receptor level↑ -Free estrogen / free testosteron↑
ETIOLOGIC FACTORS CONT‘ • Role of Androgens Major trigger of BPH 5α reductase Testosteron Dihidrotestosteron (DHT) DHT is the major intraprostatic testosteron, affinity of androgen receptors are increased
Role of Estrogens Is believed to show synergistic effect together with androgens in BPH Increases count of androgen receptors (?) Increases transformation of testosteron to DHT, thus increases prostatic DHT level (?)
Stromal/Epithelial reaction, supported by androgens, is known to have an effect in prostate formation in an embryo • Mitotic effect of androgens is only possible if stromal cells are present
5α reductase enzyme is mostly found in the stromabut tissue culutures have androgens to cause growth of epithelias cells only in presence of stromal cells • This supports the action-reaction of stromal/epithelial cells
Stromal cells‘ regulatory effect on epithelial growth is supported by studies showing paracrine mechanism and several growth factors effecting proto-oncogenes
GROWTH FACTORS IN BPH • Keratinocytegrowth factor (KGF) • Epidermal growth factor (EGF) • Insulin likegrowth factor (IGF-1/2) • Fibroblast growth factor (FGF) • Transforming growth factor (TGF)
RESULTS • BPH occurs with increasing age related hormonal changes, effect of GF within peptide structure and the reactivation of embryonic growth potential of stroma
GENETICS • Genetic predisposition BPH Familial Sporadic 1-Family history of 3 or more 1-Prostate Volume affected family members (mean age 55.5) 2- Early onset ( surgery under 60 y/a) 3-Increased prostatic volume (average 82.7)
OBSTRUCTION CAUSES • 3 steps • Anatomic obstruction • Prim. pathophysiologic obstruction (high pressure proximal to obstruction) • Second. pathophysiologicobstruction (retention - infection – hydronephrosis)
BPH’da Üretradaki Değişiklikler DEFORMATION ELONGATION DEVIATION
BLADDER RESPONSE TO OBSTRUCTION • Early stage • Compensatorystage • Decompensatorystage
Compensatory Stage • Trabeculation • Cellule • Diverticule
Decompensatory stage • Muscle tissue is replaced by connective tissue • Emptying function progressively decreases • Compliance decreases • Increased pressure • Detrusor instability
Advanced stage upper urinary system • Bilateral ureterectasia • Ureterohydronephrosis • Chronic kidney failure
CLINIC As the prostate grows, symptoms and urine flow rate deteriorate. Some patients present with acute urinary retention, needing emergency surgery !!!!BPH IS MOSTLY PROGRESSIVE!!!!
COMPLICATIONS • Acute urinary retention • Urinary system infection • Bladder stones • Bladder damage • Renal failure • Hematuria
DIAGNOSIS • History • Score of symptoms • Physical examination • Digital rectal exam,neurologic examination • Urinary diary • Complete urinanalysis • Creatinin • PSA ?? • Urine stream speed • PMR
SYMPTOMS OF BPH Irritative • Nocturia • Pollakuri • Disuria • Urgency Obstructive • ↓ urinary stream speed • Difficulty/delay starting urination • Postmictionaldrops • Sensation of not fully emptying • Urinary retention • Overflow incontinence
SCORES FOR BPH • Boyarsky • AUA • I-PSS • I-PSS (turkish score)
IPSS • Score rates between 0-35 • 0-7 mild, • 8-19 moderate, • 20-35 advanced lower urinary system signs
LABs AND RADIOLOGIC EXAM • Urinanalysis,Creatinin • PSA • UltrasonographyUrinary Transrectal • IVP • Uroflowmetry
URINANALYSIS • Show hematuria and infections if present
Kreatinin • Creatinineelevation may increase risk of post-op complications • Preoperative Creatinine measurement is recommended
PSA • Prostate specific antigen (PSA) is a protease (glycoprotein) excreted by epithelial • BPH may cause a moderate elevation in PSA • Normal ? 4? 2.5?
PSA • Between 50-70y, annual PSA&DRE check • If family history, PSA&DRE at 4th decade
USG or IVP • Hematuria, history of renal stones, history of UTI,history ofurogenital surgery ve kidney function deterioration requires USG or IVP
IVP Prostatic indentation - fishing hook sign - bladder stone - increased trabeculation, cellules and diverticules - Post- voiding imaging showing residual urine