Download
1 / 1
10 likes | 121 Views
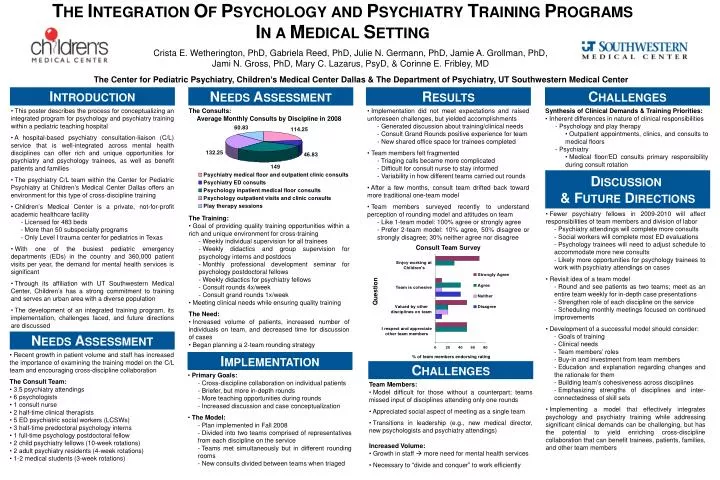
Crista E. Wetherington, PhD, Gabriela Reed, PhD, Julie N. Germann, PhD, Jamie A. Grollman, PhD, Jami N. Gross, PhD, Mary C. Lazarus, PsyD, & Corinne E. Fribley, MD.

E N D
Crista E. Wetherington, PhD, Gabriela Reed, PhD, Julie N. Germann, PhD, Jamie A. Grollman, PhD, Jami N. Gross, PhD, Mary C. Lazarus, PsyD, & Corinne E. Fribley, MD The Center for Pediatric Psychiatry, Children’s Medical Center Dallas & The Department of Psychiatry, UT Southwestern Medical Center INTRODUCTION NEEDS ASSESSMENT RESULTS CHALLENGES • This poster describes the process for conceptualizing an integrated program for psychology and psychiatry training within a pediatric teaching hospital • A hospital-based psychiatry consultation-liaison (C/L) service that is well-integrated across mental health disciplines can offer rich and unique opportunities for psychiatry and psychology trainees, as well as benefit patients and families • The psychiatry C/L team within the Center for Pediatric Psychiatry at Children’s Medical Center Dallas offers an environment for this type of cross-discipline training • Children’s Medical Center is a private, not-for-profit academic healthcare facility • Licensed for 483 beds • More than 50 subspecialty programs • Only Level I trauma center for pediatrics in Texas • With one of the busiest pediatric emergency departments (EDs) in the country and 360,000 patient visits per year, the demand for mental health services is significant • Through its affiliation with UT Southwestern Medical Center, Children’s has a strong commitment to training and serves an urban area with a diverse population • The development of an integrated training program, its implementation, challenges faced, and future directions are discussed • The Consults: • Average Monthly Consults by Discipline in 2008 • The Training: • Goal of providing quality training opportunities within a rich and unique environment for cross-training • Weekly individual supervision for all trainees • Weekly didactics and group supervision for psychology interns and postdocs • Monthly professional development seminar for psychology postdoctoral fellows • Weekly didactics for psychiatry fellows • Consult rounds 4x/week • Consult grand rounds 1x/week • Meeting clinical needs while ensuring quality training The Need: • Increased volume of patients, increased number of individuals on team, and decreased time for discussion of cases • Began planning a 2-team rounding strategy • Implementation did not meet expectations and raised unforeseen challenges, but yielded accomplishments • Generated discussion about training/clinical needs • Consult Grand Rounds positive experience for team • New shared office space for trainees completed • Team members felt fragmented • Triaging calls became more complicated • Difficult for consult nurse to stay informed • Variability in how different teams carried out rounds • After a few months, consult team drifted back toward more traditional one-team model • Team members surveyed recently to understand perception of rounding model and attitudes on team • Like 1-team model: 100% agree or strongly agree • Prefer 2-team model: 10% agree, 50% disagree or strongly disagree; 30% neither agree nor disagree • Consult Team Survey • Synthesis of Clinical Demands & Training Priorities: • Inherent differences in nature of clinical responsibilities • Psychology and play therapy • Outpatient appointments, clinics, and consults to medical floors • Psychiatry • Medical floor/ED consults primary responsibility during consult rotation DISCUSSION & FUTURE DIRECTIONS • Fewer psychiatry fellows in 2009-2010 will affect responsibilities of team members and division of labor • Psychiatry attendings will complete more consults • Social workers will complete most ED evaluations • Psychology trainees will need to adjust schedule to accommodate more new consults • Likely more opportunities for psychology trainees to work with psychiatry attendings on cases • Revisit idea of a team model • Round and see patients as two teams; meet as an entire team weekly for in-depth case presentations • Strengthen role of each discipline on the service • Scheduling monthly meetings focused on continued improvements • Development of a successful model should consider: • Goals of training • Clinical needs • Team members’ roles • Buy-in and investment from team members • Education and explanation regarding changes and the rationale for them • Building team’s cohesiveness across disciplines • Emphasizing strengths of disciplines and inter-connectedness of skill sets • Implementing a model that effectively integrates psychology and psychiatry training while addressing significant clinical demands can be challenging, but has the potential to yield enriching cross-discipline collaboration that can benefit trainees, patients, families, and other team members Question NEEDS ASSESSMENT • Recent growth in patient volume and staff has increased the importance of examining the training model on the C/L team and encouraging cross-discipline collaboration • The Consult Team: • 3.5 psychiatry attendings • 6 psychologists • 1 consult nurse • 2 half-time clinical therapists • 5 ED psychiatric social workers (LCSWs) • 3 half-time predoctoral psychology interns • 1 full-time psychology postdoctoral fellow • 2 child psychiatry fellows (10-week rotations) • 2 adult psychiatry residents (4-week rotations) • 1-2 medical students (3-week rotations) IMPLEMENTATION % of team members endorsing rating CHALLENGES • Primary Goals: • Cross-discipline collaboration on individual patients • Briefer, but more in-depth rounds • More teaching opportunities during rounds • Increased discussion and case conceptualization • The Model: • Plan implemented in Fall 2008 • Divided into two teams comprised of representatives from each discipline on the service • Teams met simultaneously but in different rounding rooms • New consults divided between teams when triaged • Team Members: • Model difficult for those without a counterpart; teams missed input of disciplines attending only one rounds • Appreciated social aspect of meeting as a single team • Transitions in leadership (e.g., new medical director, new psychologists and psychiatry attendings) • Increased Volume: • Growth in staff more need for mental health services • Necessary to “divide and conquer” to work efficiently