Download
1 / 59
620 likes | 1.81k Views
Carotid Pathology. Carotid - Pathology. Plaque characteristics and grading Stenosis Thrombosis/Occlusion Aneurysm Carotid Body Tumor Dissection Fibromuscular displasia Vertebral / Subclavian steal. Pathology - Plaque. Fatty Streaks Mild, moderate, or severe

E N D
Carotid - Pathology • Plaque characteristics and grading • Stenosis • Thrombosis/Occlusion • Aneurysm • Carotid Body Tumor • Dissection • Fibromuscular displasia • Vertebral / Subclavian steal
Pathology - Plaque • Fatty Streaks • Mild, moderate, or severe • Homogenous vs. heterogeneous • Smooth vs irregular • Calcified • Ulcerative • Occlusion
Plaque Characteristics Smooth and Homogeneous
Plaque Characteristics Heterogeneous/Irregular/Calcified
Plaque Characteristics Heterogeneous/Irregular/Calcified
Plaque Ulceration Sonography detection of ulcerations remains controversial. With sensitivities ranging from <30% to more than 90%.
Plaque Ulceration DX: 2x2 mm crater; filled with color.
Carotid Stenosis • Velocity flow remains normal until lumen diameter is reduced by 50% (Spectral Broadening). • Moderate (50-70%) a pressure gradient exists throughout diastole. • Severe (70-90%) increased pressure gradient = Peak Systolic & End Diastolic Velocities with Poststenotic Turbulence.
Hemodynamicaly Significant Stenosis • Greater than 70% diameter or 90% cross-sectional area reduction. • Exhibits Poststenotic Turbulence. • Peak Systolic Velocity 250 cm/sec or greater “JET” flow & End Diastolic Velocity greater than 100 cm/sec
Critical Stenosis Spectral Broadening with Forward and Reverse Components (Post Stenotic Turbulence)
Critical Stenosis Elevated PSV/EDV
Color Hallmarks Indicating Hemodynamic Stenosis Post-stenotic turbulence useful for detecting >70% decreased diameter. Forward & reverse flow components.
Color Hallmarks Indicating Hemodynamic Stenosis Tissue vibration caused by severe obstruction (Mosaic pattern).
Proximal Disease Right CCA/ICA
Proximal Disease Tardus-Parvus/Monophasic Waveforms: Right CCA/ICA
Distal Disease ICA Occlusion Ipsilateral Internalized ECA Ipsilateral High Resistance CCA Ipsilateral High Resistance ICA
Indirect Signs of Stenosis/Obstruction Stenosis obscured Jet by Calcification
Indirect Signs of Stenosis/Obstruction Poststenotic Waveform Indicates >70% Diameter Reduction
Indirect Signs of Stenosis/Obstruction High Resistance Distal Disease CCA
Indirect Signs of Stenosis/Obstruction Tardus-Parvus Proximal Disease CCA
Subtotal ICA Occlusion Low Flow Setting String Sign Power Doppler
Subtotal ICA Occlusion Ipsilateral High Resistance ICA Ipsilateral High Resistance CCA Power Doppler
Detection ICA Occlusion: • Absent flow by spectral & color imaging • Thrombus completely filling the lumen • Reverse flow in segment proximal to ICA or CCA
Detection ICA Occlusion: • High Resistance waveforms in ipsilateral CCA/Proximal ICA • Internalization of ECA • Increased velocities in contralateral CCA
Internal Carotid Artery Occlusion StumpFlow Thrombus StumpFlow ICA High Resistance CCA Color Void/Low Flow Internalization ECA
CCA Occlusion • Clinical features similar to ICA Occlusion • Incidence 1-5% of Cases (Rare) • Left side predilection (89%)
Common Carotid Artery Occlusion • ECA supplies ICA via Carotid Bifurcation • ECA flow is reversed • Ipsilateral Intracranial ICA not fully compensated by: • Vertebrobasilar Circulation • Contralateral ICA • Ipsilateral ICA flow is Antegrade/Damped
CCA - Occlusion Sonographic Findings Absent CCA Flow by Color Doppler
CCA - Occlusion Sonographic Findings Absent CCA Flow by Spectral Doppler
CCA - Occlusion ECA/ICA Reverse Flow Directions
CCA - Occlusion Sonographic Findings Antegrade/Damped ICA Flow
CCA - Occlusion Sonographic Findings Reverse Flow in ECA by Color/Spectral
CCA - Occlusion Sonographic Findings Reverse Flow in ECA by Color/Spectral
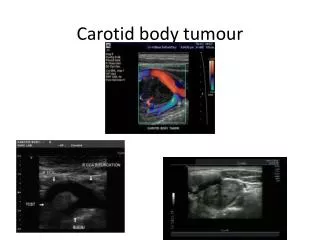
Carotid Body Tumor • Rare tumors, 1 in 30,000 in general population • Malignant potential 2-10% of cases • Palpable, painless slow growing neck mass
Carotid Body Tumor • Other signs; pain, headache, hypertension, Horner’s syndrome • Highly vascular located between the ICA & ECA • Blood supply via the ECA
Carotid Body Tumor Sonographic Findings ICA Solid well-circumscribed Hypoechoic Mass T Splaying of ICA/ECA ECA ECA Blood Supply
Carotid Body Tumor ICA Highly Vascular T ECA