Download
1 / 15
150 likes | 752 Views
Acute Achilles Tendon Rupture. Paul Herickhoff, MD March 26, 2009. Background. Largest, most powerful tendon in body Formed by gastrocnemius and soleus Incidence of rupture 18:100,000 Incidence is increasing

E N D
Acute Achilles Tendon Rupture Paul Herickhoff, MD March 26, 2009
Background • Largest, most powerful tendon in body • Formed by gastrocnemius and soleus • Incidence of rupture 18:100,000 • Incidence is increasing • As demonstrated by population based studies in Finland, Canada, Scotland and Sweden
Presentation • Adults 40-50 y.o. primarily affected (M>F) • Athletic activities, usually with sudden starting or stopping • “Snap” in heel with pain, which may subside quickly
Factors to consider • 25% of patients have previous symptoms of Achilles inflammation • Leppilahti et al. Clin Orthop 1998 • Associated conditions: • Ochronosis • Steroid use • Quinolones • Inflammatory arthritis
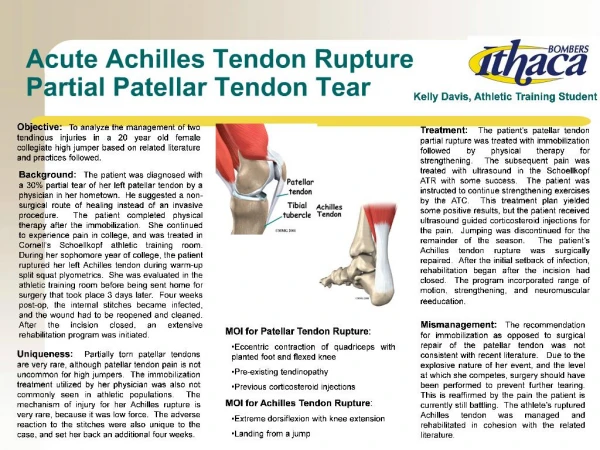
Diagnosis • Weakness in plantarflexion • Gap in tendon • Positive Thompson test
Imaging • X-rays • Indicated if fracture or avulsion fracture suspected • Ultrasound or MRI • Reveal tendon degeneration, if present
Treatment • Non-operative versus operative treatment controversial • Several methods described for each
Non-operative • Cast immobilization • Traditional recommendation is 8 weeks of immobilization • Wallace recommended patellar tendon bearing orthosis for weeks 4-8 • Functional brace with semi-rigid tape and polypropylene orthoses for duration of treatment also described • Rerupture rate 8-39% reported
Operative • Open repair • Locking stitch, +/- augmentation with plantaris or mesh • Post-op care = Casting for 6-8 weeks • Risks: Infection (4-21%), Rerupture (1-5%)
Operative • Percutaneous • Bunnell stitch • Weaker than open repair (Rerupture 0-17%) • Risk of sural nerve injury (0-13%) • Decreased infection risk
Op vs. Non-op • Wong et al Am J Sports Med 2002 • Metanalysis 125 articles, 5370 patients • Wound complication (14.6 vs 0.5%) • Rerupture (1.5 perc,1.4 open vs 10.7%) • Complication rates lowest in open repair and early mobilization, highest in percutaneous repair and early mobilization
Op vs. Non-op • Bhandari et al. Clin Orthop 2002 • More stringent inclusion criteria than Wong • 6 studies, 448 patients • Wound infection (5% vs 0%) • Rerupture (3% vs 13%)
Risk Factors for Wound Complication • Bruggeman et al Clin Orthop 2004 and Pajala et al. JBJS 2002 • Age • Tobacco • Diabetes • Female gender • Steroid use • Treatment delay • Low energy injury (during ADL’s)
Summary • Incidence of Achilles tendon rupture increasing • Operative repair associated with lower rerupture rate, but higher wound complication rate compared to non-op • Percutaneous repair has risk of nerve injury • Review risk factors before deciding treatment plan
References • Bhandari, M et al. “Treatment of Achilles tendon ruptures: a systematic overview and metaanalysis.” Clin Orthop 400:190-200, 2002. • Bruggeman, NB et al. “Wound complications after open Achilles tendon repair: an analysis of risk factors.” Clin Orthop 427:63-66, 2004 • Chiodo, CP and MG Wilson. “Current Concepts Review: Acute Ruptures of the Achilles Tendon.” Foot Ank Int 27:305-13, 2006 • Leppilahti J et al. “Outcome and prognostic factors of Achilles rupture using a new scoring method. Clin Orthop 346:152-61, 2001. • Pajala, A et al. “Rerupture and deep infection following treatment of total Achilles rupture.” JBJS 84-A:2016-21, 2002. • Wong, J et al. “Quantitative review of operative and nonoperative management of Achilles tendon ruptures. Am J. Sports Med. 30:565-75, 2002.