Download
1 / 43
470 likes | 1.4k Views
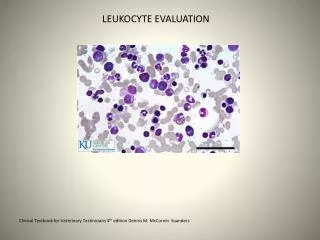
NONMALIGNANT LEUKOCYTE DISORDERS. NONMALIGNANT LEUKOCYTE DISORDERS. Changes in leukocyte concentration and morphology often reflect disease processes and toxic challenge. The type of cell affected depends upon its primary function:

E N D
NONMALIGNANT LEUKOCYTE DISORDERS • Changes in leukocyte concentration and morphology often reflect disease processes and toxic challenge. • The type of cell affected depends upon its primary function: • In bacterial infections, neutrophils are most commonly affected • In viral infections, lymphocytes are most commonly affected • In parasitic infections, eosinophils are most commonly affected.
NONMALIGNANT LEUKOCYTE DISORDERS • Neutrophil disorders • The peripheral neutrophil concentration depends upon • Bone marrow production and release • The rate of neutrophil movement into the tissues • The proportion of circulating to marginating neutrophils • Most benign quantitative abnormalities occur in response to physiologic or pathologic processes • Neutrophilia – an increase in neutrophils • Immediate – may occur without tissue damage or other pathologic stimulus. • Results from a simple redistribution of cells from the marginal pool to the circulating pool
NONMALIGNANT LEUKOCYTE DISORDERS • May occur after violent exercise, epinephrine administration, anesthesia, or anxiety • Is also called shift neutrophilia • Acute neutrophilia – this occurs 4-5 hours after a pathologic stimulus • Results from an increased flow of cells from the bone marrow to the peripheral blood • Bands and metamyelocytes may be seen • Chronic neutrophilia – this follows acute neutrophilia • The bone marrow starts to throw out younger and younger cells (a shift to the left)
NONMALIGNANT LEUKOCYTE DISORDERS • Conditions that are associated with neutrophilia are: • Bacterial infections (most common cause) • This usually causes an absolute neutrophilia (10-19 x109/L) • In severe infections, the bone marrow stores may be depleted and this can result in neutropenia (typically seen in typhoid fever and brucellosis) • Tissue destruction or drug intoxication (tissue infarctions, burns, neoplasms, uremia, gout)
NONMALIGNANT LEUKOCYTE DISORDERS • Leukemoid reaction – this is an extreme neutrophilia with a WBC count > 30 x 109/L • Many bands, metamyelocytes, and myelocytes are seen • Occasional promyelocytes and myeloblasts may be seen. • This condition resembles a chronic myelocytic leukemia (CML), but can be differentiated from CML based on the fact that in leukemoid reactions: • There is no Philadelphia chromosome • The condition is transient • There is an increased leukocyte alkaline phosphatase score (more on this later) • Leukemoid reactions may be seen in tuberculosis, chronic infections, malignant tumors, etc.
NONMALIGNANT LEUKOCYTE DISORDERS • Leukoerythroblastic reaction – in this condition nucleated RBCs and neutrophilic precursors are both found in the peripheral blood • The WBC count may be increased, normal, or decreased • This is associated with myelopthesis (proliferation of abnormal elements in the bone marrow) • Reactive states • With hemorrhage or hemolysis of RBCs, there is increased production of RBCs in the bone marrow and sometimes the granulocyte production also increases. • Corticosteroid therapy
NONMALIGNANT LEUKOCYTE DISORDERS • Neutropenia – this may result from • Decreased bone marrow production • The bone marrow will show myeloid hypoplasia with a decreased M:E ratio • The bone marrow storage pool, and peripheral and marginating pools are all decreased • Immature cells may be thrown into the peripheral blood and those younger than bands are ineffective at phagocytosis. This can lead to overwhelming infections. • This may be due to stem cell failure, radiotherapy, chemotherapy, or myelopthesis. • Ineffective bone marrow production • The bone marrow will be hyperplastic • Defective production is seen in megaloblastic anemias and myelodysplasic syndromes where the abnormal cells are destroyed before they are released from the bone marrow
NONMALIGNANT LEUKOCYTE DISORDERS • Increased cell loss • Early in an infection there is a transient decrease due to increased movement of cells into the tissues • Could be due to an immune mechanism such as production of anti-leukocyte antibodies or PNH • Hypersplenism • Pseudoneutropenia – alterations may occur in the circulating to marginating pools. This may be seen in: • Early in any infection: • Viral infections • Bacterial infections with endotoxin production • Hypersensitivity reactions
NONMALIGNANT LEUKOCYTE DISORDERS • Periodic or cyclic – is an inherited autosomal dominant disorder in which every 21-30 days there are several days of neutropenia with accompanying infections. This is followed by asymptomatic periods. • Familial – this is benign, chronic, and mild with rare clinical symptoms • Infantile genetic agranulocytosis – this is a rare, congenital, and often fatal disorder in which there is defective bone marrow production of neutrophils. • False – blood drawn into EDTA in which the cells stick to the side of the tube; disintegration of cells due to age from sitting in a tube for too long; cell clumping
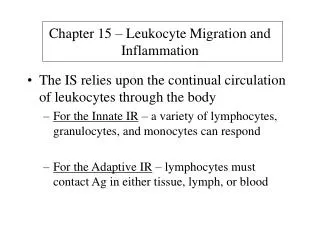
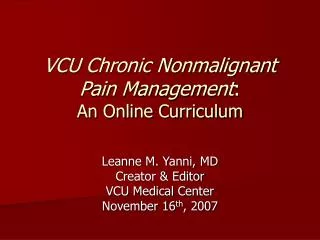
NONMALIGNANT LEUKOCYTE DISORDERS • Morphologic and functional abnormalities of neutrophils • Acquired, morphologic – these are reactive, transient changes accompanying infectious states. They include • Toxic granulation • Dohle bodies • Cytoplasmic vacuoles • May also see ingested microorganisms
MORPHOLOGIC NEUTROPHIL CHANGES Vacuolated cell
MORPHOLOGIC NEUTROPHIL CHANGES Toxic granulation
NONMALIGNANT LEUKOCYTE DISORDERS • Inherited functional and/or morphological abnormalities • Pelger- Huet Anomaly – this is a benign, inherited, autosomal dominant abnormality in which the neutrophil nucleus does not segment beyond the bilobular stage (“Prince-nez cells”). • The cells may sometimes resemble bands, but the chromatin is more condensed (mature). • The cells function normally. • Acquired or pseudo Pelger-Huet Anomaly is seen in myeloproliferative and myelodysplastic states
PSEUDO PELGER-HUET ANOMALY Note nuclear maturity
NONMALIGNANT LEUKOCYTE DISORDERS • Alder-Reilly Anomaly – in this disorder all leukocytes contain large, purplish granules (due to partially degraded protein-carbohydrates) in the cytoplasm, but the cells function normally. • This is seen in Hurler’s and Hunter’s syndromes in which there is an incomplete breakdown of mucopolysaccharides
HURLER’S SYNDROME Note the granules
NONMALIGNANT LEUKOCYTE DISORDERS • Chediak-Higashi Anomaly – • This is a rare autosomal recessive disorder in which abnormal lysosomes are formed by the fusion of primary granules. These are seen as grayish-green inclusions • The cells are ineffective in killing microorganisms and affected individuals often die early in life from pyogenic infections.
CHEDIAK-HIGASHI ANOMALY Note abnormal lysosomes
NONMALIGNANT LEUKOCYTE DISORDERS • May-Hegglin Anomaly • This is a rare, autosomal dominant disorder in which the leukocytes contain large basophilic inclusions containing RNA that look similar to Dohle bodies. • It can be differentiated from an infection because toxic granulation is not seen. • The patients also have giant platlets that have a shortened survival time. Because of this, patients may have bleeding problems, but they usually have no other clinical symptoms
NONMALIGNANT LEUKOCYTE DISORDERS • Chronic granulomatous disease • This is a lethal, sex-linked disorder affecting the function of the neutrophil • The neutrophil can function in phagocytosis, but it cannot kill microorganisms because the cells have a defect in the respiratory burst oxidase system. • Affected individuals have chronic infections with organisms that do not normally cause infections in normal individuals • Myeloperoxidase deficiency • This is a benign, autosomal recessive disorder characterized by a lack of myeloperoxidase in the neutrophils
NONMALIGNANT LEUKOCYTE DISORDERS • Affected individuals may have occasional problems with Candida infections, but usually they have no problems with infections because they have other mechanisms to kill microorganisms • Leukocyte adhesion deficiency • This is a rare, autosomal recessive disorder characterized by the absence of leukocyte cell surface adhesion proteins • Because of the lack of the adhesion molecules, the leukocytes have functional defects in: • Chemotaxis • Phagocytosis • Respiratory burst activation • Degranulation • Affected individuals have frequent bacterial and fungal infections and mortality in childhood is high.
NONMALIGNANT LEUKOCYTE DISORDERS • Eosinophil disorders • Eosinophilia may be found in • Parasitic infections • Allergic conditions and hypersensitivity reactions • Eosinophils have low affinity IgE Fc receptors and may be important in modulating immediate hypersensitivity reactions • Cancer • Chronic inflammatory states
NONMALIGNANT LEUKOCYTE DISORDERS • Basophil disorders • Basophilia • Is associated with chronic myeloproliferative disorders (discussed later) • Inflammatory bowel disease • Radiation exposure • Monocyte quantitative and qualitative disorders • Associated with malignancies
NONMALIGNANT LEUKOCYTE DISORDERS • Inherited abnormalities of neutrophils are also seen in monocytes because they originate from a common stem cell: • Chronic granulomatous disease (defective respiratory burst) • Chediak Higashi (abnormal lysosomes caused by fusion of primary granules) • Alder Reilly Anomaly (large purple-blue granules)
NONMALIGNANT LEUKOCYTE DISORDERS • Macrophage disorders • Lipid storage diseases – the cells are unable to completely digest phagocytosed material • Gaucher’s disease – is a recessive autosomal disorder with a deficiency of glucocerebroside • There is an accumulation of lipid in macrophages in lymphoid tissue • This leads to liver and spleen enlargement and destructive bone marrow lesions • Death occurs early in life
NONMALIGNANT LEUKOCYTE DISORDERS • Niemann-Pick Disease – This is an autosomal recessive disorder with a defect in sphingomyelinase • It is often fatal by the age of 3 • Tay Sachs and Sandhoffs diseases – these are autosomal recessive disorders with deficiencies in - hexosaminidase and and - hexosaminidase, respectively • Gangliosides and other glycolipids and mucopolysaccharides accumulate in tissues, especially in the CNS. • This is usually fatal by the age of 4 • Fabry’s, Wolman’s, and Tangier are examples of other lipid storage diseases
NONMALIGNANT LEUKOCYTE DISORDERS • Lymphocyte disorders • Acquired, quantitative • Is usually a self-limited reactive process to infection or inflammation • Both B and T cells are affected • Function is normal, though the morphological process may be heterogenous • With intense proliferation, may have lymphadenopathy or splenomegaly
NONMALIGNANT LEUKOCYTE DISORDERS • Lymphocytosis – may be relative (secondary to neutropenia) or absolute (usually seen in viral infections); if absolute it may or may not be accompanied by a leukocytosis • Infectious mononucleosis (IM) – • This is caused by Epstein-Barr virus infecting B lymphocytes. • The infected B cells may eventually be killed by cytotoxic T cells, though some will continue to harbor the virus in a latent infection. • The reactive lymphocytes seen in the peripheral smear are cytotoxic T cells • The lymphocytosis is accompanied by a leukocytosis
NONMALIGNANT LEUKOCYTE DISORDERS • Cytomegalovirus infection • Leukocytosis with absolute lymphocytosis • Infectious lymphocytosis • Unknown etiology • Leukocytosis with absolute lymphocytosis • 60-97% normal appearing lymphocytes • The increased lymphocytes are mainly T lymphs • Bordetella pertussis infection • Leukocytosis with an absolute lymphocytosis • Due to a redistribution of T lymphocytes from the tissues to the circulation • Lymphocytes are small, normal appearing lymphocytes
NONMALIGNANT LEUKOCYTE DISORDERS • Lymphocytic leukemoid reaction – • Peripheral smear shows increased lymphocytes with younger lymphocytes being seen • Can occur with tuberculosis, chickenpox and the viral diseases discussed above • Plasmocytosis • Plasma cells are rarely seen in the peripheral blood, but they may be found under conditions of intense immune stimulation • Lymphocytopenia – caused by stress, drugs, irradiation, and some diseases
NONMALIGNANT LEUKOCYTE DISORDERS • Congenital qualitative or quantitative disorders – may affect both T and B cells or only one cell type. Most will severely compromise the immune system • Severe combined immunodeficiency system (SCIDS) • This is a heterogenous group of disorders in which both B and T cells are profoundly deficient • In some cases there is no rearrangement of the B cell and T cell receptor genes to produce immunocompetent cells • A bone marrow transplant or gene therapy are the only effective treatments
NONMALIGNANT LEUKOCYTE DISORDERS • Wiskott-Aldrich Syndrome • Is a sex-linked progressive disorder characterized by • Eczema • Thrombocytopenia • Immunodeficiency due to progressive decrease in T cell immunity • There is also an intrinsic B lymphocyte abnormality resulting in an inability to respond to polysaccharide antigens • Most children die before the age of 10 from bleeding and infections • Treatment is a bone marrow transplant
NONMALIGNANT LEUKOCYTE DISORDERS • DiGeorge syndrome • This is characterized by absence or aplasia of the thymus and parathyroid gland • This results in decreased T lymphocytes and death in the first year without thymic grafts • X linked agammaglobulinemia • This is characterized by a block in B lymphocyte maturation leading to a decrease in B lymphocytes and no plasma cells • There is decreased IgM, IgA, and IgG • Treatment is monthly injections with gammaglobulin to prevent infections • Ataxia telangiactasia • This is a cell mediated immune defect with thymic hypoplasia or dysplasia and depletion of T cells
NONMALIGNANT LEUKOCYTE DISORDERS • Acquired immune deficiency syndrome (AIDS) • Caused by human immunodeficiency virus (HIV) • Viral infection results in a selective depletion of T helper cells resulting in opportunistic infections