Download
1 / 18
180 likes | 299 Views
Osteoarthritis and Total Joint Replacement. Risk Factors, Prevention, and Treatment, and the Effects on Sensory Mechanisms Encountered by Osteoarthritic Total Joint Replacement Patients. Neil V. Shah BioNB 4210, Fall 2008 Final Project. An Introduction to Osteoarthritis.

E N D
Osteoarthritis and Total Joint Replacement Risk Factors, Prevention, and Treatment, and the Effects on Sensory Mechanisms Encountered by Osteoarthritic Total Joint Replacement Patients Neil V. Shah BioNB 4210, Fall 2008 Final Project
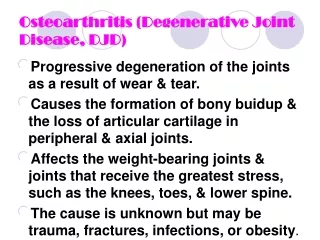
An Introduction to Osteoarthritis • Osteoarthritis (OA) is a slow-progressing joint inflammation that can result from cartilage degeneration. • OA is the most common form of arthritis, even more common as age increases. Nearly 27 million Americans older than 25 years of age have OA. • By 2030, nearly 20% of Americans (approximately 72 million people) will surpass 65 years of age and be at high risk for OA. • Under the age of 45, male OA patients outnumber females. After that age, it is more common in women. It is also more likely to develop in overweight people and people with jobs that stress certain joints.
What Does OA Affect? • OA onset at where joints occur, most commonly affecting the hands and finger-ends, neck, lower back, knees, and hips (Figure 1, left). • It is painful and can negatively influence lifestyle, bringing on depression and a sense of helplessness, and finances, as treatment options can be expensive. • It is also a very common cause for falls in the elderly. It leads to weakened bone and muscle strength, and this can severely worsen the effects of a fall on an elderly person. Figure 1. (Backside Body View) Courtesy of NIH NAMS
An Osteoarthritic Joint • Two types of OA: • Primary OA: attributed to age, heredity, and activity-related deterioration on joint cartilage, resulting in a total loss of cartilage cushion between the bones of joints (Figure 2 above). • Secondary OA: caused by other diseases/co-morbidities, such as obesity, trauma, diabetes, etc. Figure 2. Courtesy of Shiel 2008, MedicineNet
Symptoms & Diagnosis of OA • Frequently, OA patients complain of: • Stiffness in a joint after getting out of bed or sitting for a long time • Swelling and pain in one or more joints • A Crunching feeling or the sound of bone rubbing on bone **If your skin turns red or you feel hot, you may not have OA; it could be of another cause, such as rheumatoid arthritis • Common Ways to Diagnose OA • Patient’s Clinical History and Physical Exam • X-rays (Figure 3, right) or MRI images read by an Orthopedist Figure 3. Courtesy of CentraCare
Effective Treatments for OA • Goals of Treatment • Control Pain • Improve Joint Function • Treatment Options • Exercise • Strengthening, Aerobic, Agility • Weight Control • Surgery • Complementary Methods • Acupuncture • Nutritional Supplements • Restore Lifestyle • Maintain Normal Weight • Pain Medications • Acetaminophen • Corticosteroids • Hyaluronic Acids
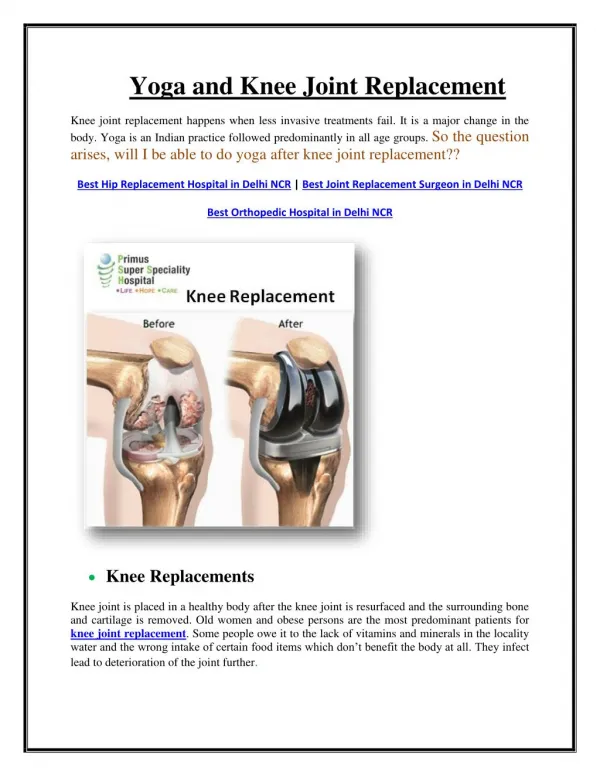
Surgery • Total Joint Replacement (TJR) • Prosthetic devices made from metal alloys (Figure 4, below), high-density plastic, or ceramic material used to replace severely affected joints. Can be performed for degraded hips, knees, shoulders, and ankles. • Artificial joints have become increasingly long-lasting (up to 10-15 years). May require revision or re-replacements after that time. • Joint Resurfacing • The surfaces of the bones in the joint can be surgically resurfaced, or smoothed out. • In regular replacement, the head of the joint is removed, but in resurfacing, usually performed in the hip, the head is resurfaced and capped with an implant that will slide into the corresponding implanted cup. • Often a temporary step for those who avoiding or delaying open surgical intervention (replacement, etc.) or arthroscopy. Figure 4. Courtesy of DePuy Orthopaedics Shoulder Ankle Knee Hip
Surgery Cont’d • Arthroscopy • Viewing scope inserted into the joint, allowing a surgeon to view and detect the site of damage (Figure 5, below) • Sometimes this can be can repaired through an arthroscope. • Often a successful procedure with recovery time quicker than open joint surgery. Figure 5. Courtesy of Essex Knee Surgery
Joint Replacement • Who Can Help You Treat your OA? • In addition to major orthopedic hospitals, many community hospitals can now perform not only therapeutic treatment but surgeries. • Primary Care Physicians • Rheumatologists • Orthopaedists • Physical Therapists • Occupational Therapists • Nurse Educators • Dieticians • Physiatrists (Rehab Specialists) • Licensed Acupuncture Therapists • Psychologists • Social Workers
More on Joint Replacement • This procedure is continually improving itself, and new methods are published frequently. • Joints can now be customized to the lifestyle and age of the patient • Middle-Aged (40-60) Athletes, Factory Workers, Frequent Travelers, etc. • Orthopaedic Centers Specializing in Joint Replacement • Hospital for Special Surgery, New York, NY • NYU Hospital for Joint Diseases, New York, NY • Mayo Clinic, Rochester, MN • Cleveland Clinic, Cleveland, OH • Duke University Medical Center, Durham, NC
Tips for Those Considering Joint Replacement • Take Painkillers Before Surgery • Inform your physician • Studies in knee replacements have documented reduced pain and other postoperative effects • Request Inpatient Rehabilitation Soon after the Operation • Studies have shown that patients moved to rehab as early as three days following surgery have had successful recoveries and reduced hospital costs. • Don’t Sit on OA; Approach It In the Long-Term • Don’t wait for symptoms to become debilitating to act • Studies show that surgeries performed at later stages of joint deterioration due to OA result in worse postoperative functional status
Falls Can Accelerate Need for Surgery • Common Causes of Falls • Degraded bone density and muscle strength in the hip, knee, and ankle joints. • Changes in Visual System • Age-related changes in sight, such as hardening, yellowing, and clouding of eye lens, decrease in pupil diameter, clouding of intraocular fluids, weakened eye muscles all contribute to decline in sight • Among hip fracture patients, vision impairment is more frequent than in people without hip fractures • Changes in Perceptual and Auditory-Vestibular Systems • Declining ability to detect information combining touch and kinesthetic data (haptic perception) hurts ability to properly grasp and manipulate objects • Vestibular system, located in the ear, is vital to maintaining and coordinating balance. Age-related changes to these systems hurts ability to adapt to environmental changes or obstacles and greatly increases the risk of falling
Alternatives to Operative Treatment • Therapeutic • Use of Non-Steroidal Anti-inflammatory Drugs (NSAIDs) • Aspirin, Ibuprofin (Motrin), and Naproxen (Naprosyn) • Physical Therapy • Treatment with food supplements (glucosamine & chondroitin) • Hyaluronic Acid Injections – restores thickness of joint fluid for better joint lubrication and impact capability • Self-Managed • Rest, Exercise, Diet Control with Weight Reduction, Adjustment of Home (Showers, Stairwells, Chairs, etc.) • Complementary and Alternative Methods (CAM) • Acupuncture – by inserting fine needles into skin at specific points on body, they help reduce pain and improve physical function.
What Can You Do To Prevent OA? • Self-Care and Good Health Attitude are Vital • Get Educated about OA and how it can affect your life. You should be aware of its frequency of occurrence and thus prepare accordingly. • If you have it, join patient education programs or self-management programs to help understand and cope with OA and reduce pain • Stay Active with exercise and regular activity • Eat Well and Control Your Weight • Stay Positive – OA can be successfully managed, and research is continuing to improve the lives of OA patients on a daily basis
Intended Audience This presentation is primarily intended for elderly patients who want a generaloverview of the risk factors, symptoms, and treatmentmethods associated with osteoarthritis. It also may be useful for: • People wanting to gain a basic understanding of OA • Patients younger than 60 years of age suffering from OA • Family members of OA patients wanting to learn more about their loved ones’ conditions and ways they can help • This presentation is not intended to serve as a scientific review of OA nor is it intended to provide information that would be entirely novel to members of academia and medicine. It is merely a resource meant primarily for patient education.
References and Resources • Helpful Resources • Best Hospitals: Orthopedics. 2008. America’s Best Hospitals. US News. Dec. 4, 2008. <http://www.usnews.com/directories/hospitals/index_html/specialty+ihqorth> • Buckelew K. (2007) New technology allows joint replacement on younger patients. Daily Record. Dec. 4, 2008. <http://findarticles.com/p/articles/mi_qn4183/is_20071119/ai_n21125849/pg_1?tag=artBody;col1> • Kulkarni S. (2006) Falls And The Elderly: An Educational Resource. Dec. 4, 2008. <http://courses.cit.cornell.edu/psych431_nbb421/student2006/ssk34/whyfallsoccur.htm> • Osteoarthritis. 2002-2006. NIH NIAMS. Dec. 4, 2008. <http://www.niams.nih.gov/Health_Info/Osteoarthritis/default.asp> • Shiel, WC. Osteoarthritis. Sep. 2008. MedicineNet. Dec. 4, 2008. <http://www.medicinenet.com/osteoarthritis/article.htm#Whatis> • Images • Figure3: Thompson, EG. (2007) X-ray of osteoarthritis of the knee. CentraCare Health System. Dec. 4, 2008. <http://64.143.176.9/library/healthguide/en-us/support/topic.asp?hwid=zm6052> • Figure 4. Joint Replacement Technology. 2002-2008. DePuy Orthopaedics. Dec. 4, 2008. <http://www.jointreplacement.com/DePuy/index.html>
References and Resources Cont’d • Images Cont’d • Figure 5. Rees C. (2008) Anterior cruciate ligament (ACL) reconstruction. Essex Knee Surgery. Dec. 4, 2008. <http://www.essexkneesurgery.co.uk/anterior-cruciate-ligament-reconstruction.php> Relevant Studies and Publications (May Require Access to University Library Proxy; Can All be accessed through Respective University Library through Google Scholar) • Buvanendran A, Kroin, JS, Truman K, et. al. (2003) Effects of Perioperative Administration of a Selective Cyclooxygenase 2 Inhibitor of Pain Management and Recovery of Function After Knee Replacement.JAMA. 290: 2411 – 2418. http://jama.ama-assn.org/cgi/content/abstract/290/18/2411?ijkey=2037eae3f1d3b24c17bdf39eab0df590547a26ae&keytype2=tf_ipsecsha • Fortin PR, Clarke AE, Joseph L, et. al. (2001) Outcomes of total hip and knee replacement: Preoperative functional status predicts outcomes at six months after surgery.Arthr. and Rheum.. 42(8): 1722 – 1728. http://www3.interscience.wiley.com.proxy.library.cornell.edu/journal/79503171/abstract?SRETRY=0 • Grue EV, Kirkevold M, Mowinchel P & Ranhoff AH. (2009) Sensory impairment in hip-fracture patients 65 years or older and effects of hearing/vision interventions on fall frequency. J. Multidiscip. Healthcare. 2: 1-11. http://www.dovepress.com/articles.php?article_id=2549
References and Resources Cont’d • McCarvill S. (2005) Essay: Prosthetics for athletes. Lancet. 366(1): S10 – S11. http://www.sciencedirect.com.proxy.library.cornell.edu/science?_ob=ArticleURL&_udi=B6T1B-4HTK0YH-6&_user=492137&_rdoc=1&_fmt=&_orig=search&_sort=d&view=c&_acct=C000022719&_version=1&_urlVersion=0&_userid=492137&md5=6fc1df7a95e13d85b1eb14e4c39d7172 • Zuckerman JD. (1998) Inpatient Rehabilitation After Total Joint Replacement. JAMA. 279: 880. http://jama.ama-assn.org.proxy.library.cornell.edu/cgi/content/full/279/11/880