Download
1 / 31
310 likes | 326 Views
This presentation aims to discuss the root causes of racial health inequities in cancer control and explore the intersectionality of racial and other disparities. It also presents potential public health, healthcare, and social interventions to address these disparities.

E N D
CANCER DOES DISCRIMINATE RACIAL DISPARTIES ACROSS THE CANCER CONTROL SPECTRUM Chris Espersen, MSPH @ChrisEspersen GaganLamba, MA, MS, MBA, CSM
Objectives • Discuss the root causes of racial health inequities; • Identify the intersectionality of racial and other disparities that exist within cancer prevention, screening, treatment and quality of life; • Discuss potential public health, health care and social interventions to address racial disparities in cancer control.
RACIAL DISPARITIES ROOT CAUSES AND INTERSECTIONALITY
Dwarf the Soul and Preserve the Body • Tuskegee • Henrietta Lacks • Mississippi Appendectomy • Misinformation campaigns
The Role of Racism in Disparities: “Medical Apartheid” Harriet Washington Segregated medical profession Separate medical facilities Unequal treatment Experimentation Racial biology of violence Pennsylvania Holmesburg Prison Community hospitals 1946 Hospital Survey and Construction Act
Shariff- Marco et al, 2010 General racism associated with: • Smoking • Binge drinking • Being overweight or obese Health care racism associated with not being up to date with screening for prostate cancer.
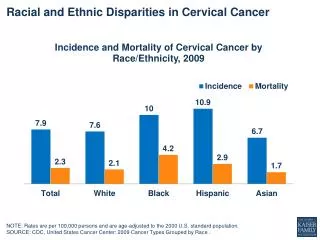
Breast and Cervical Cancer Mouton et al, 2010: Beyer et al, 2017: institutional racism is associated with an increased odds of being diagnosed with an ER-/PR- tumor
End of Life Care • Rizzuto & Aldridge, 2017 Black hospice patients were significantly more likely than white hospice patients • Be admitted to the hospital (14.9 % vs 8.7 %), • Go to the emergency room (19.8 % vs. 13.5 %), • Disenroll from hospice prior to death (18.1 % vs. 13.0 %) • Kirtane et al, 2017 hematologic malignancies • AD documentation • more aggressive care than white counterparts
“Urban Renewal” Source: Maurice Horner, Des Moines Register, April 1969
Iowa Data 2010-2014 2011-2015 38.3 39.1 40.4 45.9
What is Missing from Iowa Data? • Health behaviors • Healthcare and prevention access • Impact of racism • SDH and disparities in counties outside of Polk • Community input on strengths, barriers, and desired interventions
Commitments Given what you have heard thus far – what are you committed to doing or investigating?
Who the Iowa Primary Care Association Serves 728,625 PATIENT VISITS 203,189 TOTAL PATIENTS 3,296+ VETERANS SERVED 8,490 HOMELESS PATIENTS
Colorectal Cancer Screening – Reducing Structural Barriers • Increased awareness and communication to teams about measures, progress and changes as per population • Gas card incentive program - $10/$20 incentive to reduce barrier to screening – to all patients who complete FIT kit • Increased PR/Social media posts in March for awareness month including video about FIT test • To help with FIT test process, team including rubber gloves and hats in FIT kits, instructions in languages other than English • Added process: Triage nurse check all lab patients to see if due for screening • Health coaches used for extra encouragement of screenings to patients • Outreach assist patients who are wondering about pricing
Colorectal Cancer Screening – Reducing Structural Barriers – Improving Access with IDPH • Reducing time or distance between service delivery. • Offering FIT or FOBT at flu shot clinics. • Using patient navigators to schedule appointments, remind patients about appointments, translate information, arrange for transportation, etc. • Modifying hours of service to meet client needs. • Eliminating/simplifying administrative procedures and other obstacles (e.g., scheduling assistance, patient navigators, transportation, dependent care, translation services, limiting the number of clinic visits).
Colorectal Cancer Screening – Reducing structural barriers: Gas Card Program
Colorectal Cancer Screening – Evidence Based Interventions • Provider Reminders • Client Reminders • Provider Assessment & Feedback
Breast Cancer Project - IDPH & Iowa PCA • Breast cancer screening policies and procedures across 6 out of 11 centers • Provider recall process across 11 health centers • Improved the mammography rate tracking and reporting from 22% to 31% by implementing and integrating HIT systems at one health center • 63% centers (7 out of 11) have mammography rate tracking and reporting system implemented
What’s Next? • Increased awareness and emphasis on eliminating health care gaps for diverse populations across Iowa. • Population Health tool that displays patient level dashboard and provides actionable information
THANK YOU! espersenc@gmail.com glamba@iowapca.org