Download
1 / 95
1.29k likes | 2.44k Views
Dr.Arun Narayanaswamy Urology Unit Amiri Hospital. Benign prostatic Hyperplasia. BPH Anatomy of Prostate Aetiology Pathophysiology Incidence Clinical presentation Investigations Management. Outline. Catheterisation Indications Catheter types Technique Complications.

E N D
Dr.ArunNarayanaswamy Urology Unit Amiri Hospital Benign prostatic Hyperplasia
BPH Anatomy of Prostate Aetiology Pathophysiology Incidence Clinical presentation Investigations Management Outline Catheterisation • Indications • Catheter types • Technique • Complications
Walnut-sized. Part of male reproductive system Location Anterior to rectum, Just distal to bladder, Encircling the neck of bladder and urethra Normal weight – 20gm Anatomy of Prostate gland
Prostatic parenchyma divided into 4 Zones. Biologically and anatomical distinct. Anatomy of Prostate gland
Secretes alkaline fluid–30% of seminal volume Actions -Lubrication and nutrition for sperm, Liquefaction of the seminal plug, Neutralizes acidic vaginal environment Prevents retrograde ejaculation (ejaculation resulting in semen being forced backwards into the bladder) by closing the bladder neck during sexual climax. Functions of Prostate gland
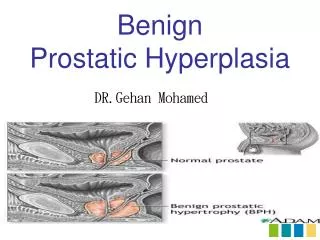
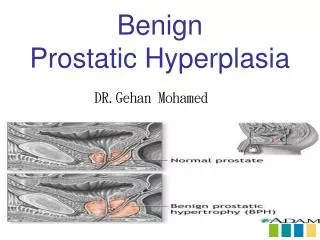
BPH is part of the natural aging process, like getting gray hair or wearing glasses Characterized by hyperplasia of prostatic stromal and epithelial cells. Occurs in the Transitional zone. Results in formation of nodules in the periurethral region of the prostate. What is BPH ?
Urethra Peripheral Zone Transition zone What is BPH ?
Aetiology of Hyperplasia • DHT-mediated hyperplasia aided by estrogens In aging men, estradiol levels increase.
Mechanism of Obstruction • Mechanical Component - When sufficiently large, the nodules compress the urethral canal
Mechanism of Obstruction • Dynamic Component - Large numbers of alpha-1-adrenergic receptors present in the smooth muscle of the stroma and capsule of the prostate, bladder neck. Stimulation causes ↑ in smooth-muscle tone
Gross - Circumscribed grey white nodules Histology Epithelial - Glandular proliferation or dilation Stromal - Fibrous or Muscular proliferation Mostly common - Fibroadenomyomatous pattern Pathology of BPH
Bladder wall - contractile force leads to: Hypertrophy or Trabeculation, and Irritability. Bladder may gradually weaken Increased residual urine volume Acute or chronic urinary retention. Biopsy - smooth-muscle fibers / in collagen - Decrease compliance, Impair contraction BPH - Bladder Effects
Prevalence of BPH • 25% - 40-49 years • 50% - 70 & older • 90% at 85 years Source: J Urol 1984;132:474 • Only 50% develop clinical symptoms. • Severity of symptoms not related to size. • Second most common surgery after cataract extraction in men > 65 years.
Common Terms • LUTS Lower-urinary-tract symptoms • BPE Benign prostatic enlargement (macroscopic) • BPH Benign prostatic hyperplasia (microscopic/histologic) • BOO Bladder-outlet obstruction
Symptoms Obstructive Symptoms (Voiding) Irritative Symptoms (Storage) - Dysuria - Frequency - Nocturia - Urgency - Incontinence - Nocturnal enuresis Elective - Weak stream - Straining to void - Hesitancy - Intermittency - Terminal dribbling - Incomplete emptying Emergency - Acute urinary retention - Chronic Retention with overflow
Symptom Assessment • International Prostate Symptom Score(IPSS) / AUA Score • Based on a survey & questionnaire developed by the American Urological Association (AUA). • 7 questions about the severity of symptoms. • Total score: Mild 0 - 7 Moderate 8 - 19 Severe 20 - 35
Studies have identified LUTS as an independent risk factor for erectile / ejaculatory dysfunction. Sexual history
Suprapubic area - Bladder distension Neurological examination - Decreased anal sphincter tone Absent bulbocavernosus reflex Palpate the scrotum: epididymoorchitis Signs of CRF, Pallor Physical Examination
Left lateral position Index finger of the dominant hand. Palpate circumferentially - windshield wiper movement Rectal Examination
Prostate size and contour, Median sulci Consistency Nodules, Hardness, Asymmetry - suggestive of malignancy. Pain - Prostatitis, Fluctuance - Prostate abscess Rectal mucosa Rectal Examination
Urinary retention • Recurrent UTIs • Gross hematuria • Bladder calculi • Bladder Diverticuli • Renal failure or uremia Complications of BPH
Urethral Strictures • Bladder Stones • Neurogenic Bladder • Prostatitis • Bladder Tumours • Radiation Cystitis • Interstitial Cystitis Differential Diagnosis
Investigations • Basic Iab: • CBC / S.Creat • Urine routine / culture • PSA(prostate specific antigen) • Xray KUB :calculi • Ultrasound • Uroflowmetry • Flexible Cystoscopy
Prostate Specific Antigen • Secreted by Prostatic cells. • Normal <4ng/dl • Marker for Carcinoma Prostate – Elevated. • BPH does not lead to prostate cancer. However men at risk for BPH are also at risk for prostate cancer and so should be screened. • Not disease specific - Also in BPH, Prostatitis,DRE,Catheterization • High PSA →Trans rectal US and Biopsy
Ultrasonography • Prostate – Size (>20cm3:abnormal), Nature • Bladder – Wall thickness, Diverticuli, Calculi • Kidneys - Hydronephrosis • Post micturition residual volume(>50-100ml)
Uroflowmetry • Simple noninvasive test to document voiding • Peak Flow rate (>15ml/s is normal) • Voiding time, Voiding pattern • Volume of voided urine – atleast 150ml
Invasive – Urethral / Rectal catheterization. Indication - To distinguish bladder contractility (detrusorunderactivity) from outlet obstruction. BOO -Low urine flow rates accompanied by High intravesical voiding pressure (>60 cm water) Cystometry - Pressure flow
Cystoscopy Flexible cystoscopy can be easily performed in an office-based setting using topical gel- intraurethralanesthesia without sedation. • Indicated when Suspicion of • Urethral stricture - h/o STD, prolonged catheterization, or trauma • Detrusorhypocontractility - DM
Treatment Options • Watchful waiting • Medical management • Surgical approaches • - Endoscopic surgery • - Minimal invasive procedures • - Open surgery
Watchful Waiting • For mild symptoms. • Follow up 1 to 2 times yearly • Suggestions that help reduce symptoms • - Avoid caffeine and alcohol • - Alteration of timing, volume of fluid intake
Medical Management Disadvantages Drug Interactions Must be taken every day Does not fix problem Side Effects Cost Benefits Convenient No loss of work time Minimal risk Types – Alpha Adrenergic Blockers 5 alpha reductase inhibitors
BPH predominantly stromal (Smooth muscle ) proliferative process - Dynamic Obstruction • Mediated by the alpha1A-adrenergic receptors. • Density of receptors changes with prostate size & age. • Alpha-adrenergic receptor-blocking agents Relax the smooth muscle Decrease outflow resistance. Alpha Blockers - Rationale
Alpha Blockers - Agents • Nonselective • - Phenoxybenzamine • Short-acting selective a1-blocker • - Prazosin, • Long-acting selective a1-blockers • - Terazosin, Doxazosin • Long-acting selective a1A-subtype • - Tamsulosin • - Alfuzosin • - Silodosin
Quick action Improves urinary flow - 4- to 6-point improvement is expected in IPSS/AUA scores No adverse effect upon sexual drive No effect on PSA Alpha Blockers - Advantages
No effect on Prostate volume No reduction in risk of acute urinary retention or BPH-related surgery. Lowers blood pressure Fatigue, nasal congestion, headache Retrograde Ejaculation Intraoperative floppy iris syndrome (IFIS) - Miosis, iris billowing, and prolapse in patients undergoing cataract surgery Alpha Blockers - Disadvantages
5 Alpha Reductase - Rationale • Prostatic growth depends on androgenic stimulation by DHT. • 5-reductase mediates conversion. • Agents that block 5-reductase inhibit growth and therefore help in BPH • Types - type I and type II • Type II predominates in the prostate and other genital tissues.
Finasteride - Selective inhibitor of type II 5-reductase • Dutasteride - Newer agent. Has affinity for both Types • Similar efficacy. • Both agents actively reduce serum DHT levels by more than 80%, 5 Alpha Reductase - Agents
Change in Prostate Volume % Change in prostate volume from baseline Dutasteride Finasteride a-blockers 30 20 10 0 -10 -20 -30 2 yrDB 4 yrOL PLESS4 yr MTOPS4 yr 6 yrOL MTOPS Dox4 yr McConnell et al. (1998); McConnell et al. (2003); Roehrbornet al. (2002); Lowe et al. (2003)
Reduce prostate volume by 20% Improve symptoms in a third of men and increase peak flow by around 2ml/s 55% reduction in incidence of urinary retention, and likelihood of surgery for BPH. Longer acting Less side effects than alpha blockers Can reverse male pattern balding 5 Alpha Reductase - Advantages
5 Alpha Reductase - Advantages • Reduce bleeding during surgery.
Slow to act - Takes up to six months to work Not effective for mildly enlarged prostates Can affect sexual function Can cause breast swelling Transmitted in semen and can cause birth defects. Users should have protected sex. Caution in liver function abnormalities Lowers serum PSA level by 50% . 5 Alpha Reductase - Disadvantages
Combination Therapy • Activates Two Distinct and Complementary Mechanisms of Action. Alpha blockers 5-Alpha reductase inhibitors Relaxes prostatic and bladder-neck smooth muscle through sympathetic activity blockadeRapidly relieve symptoms Reduces prostate enlargement through hormonal mechanisms Arrest disease progression Dutasteride+Tamsulosin / Finasteride+Tamsulosin.
Patients with prostates >30 gm. Superior to monotherapy over long term. Risk of acute urinary retention decreased by 79% - Combination therapy 31% - a-blocker alone 67% - 5a-reductase inhibitor alone. Alpha blocker may be withdrawn after 6 months Combination Therapy
Treatment of associated ED Nitric oxide known to mediate smooth muscle relaxation in the lower urinary tract. Improvements in Urinary symptoms reported Smallest necessary dose. Should not be taken within 4 hours of any alpha-blocker Phosphodiesterase 5 Inhibitors
Treatment of Frequency / Urgency. Relaxes Detrusor muscle. Historically, discouraged because of concerns of inducing urinary retention. Recommend only in patients who do not have an elevated PVR. Not to be used when PVR is greater than 250-300 mL Anticholinergics
Considered emerging therapy • Saw palmetto (American dwarf palm) Leaf • South African star grass (Hypoxisrooperi) roots • African plum tree (Pygeumafricanum) bark • Stinging nettle (Urticadioica) roots • Rye (Secalecereale) pollen • Pumpkin (Cucurbitapepo) seeds Active components - Phytosterols, Fatty acids, Lectins, Flavonoids, Plant oils, & Polysaccharides Phytotherapy