Download
1 / 78
780 likes | 954 Views
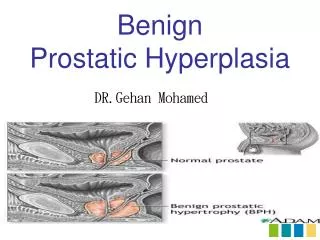
BENIGN PROSTATIC HYPERPLASIA. Zonal A natomy of the Prostate. Peripheral zone 70% of volume of young adult prostate 60-70% of CaP Central zone 25%: young adult prostate 5-10% of CaP Transition zone 5%: young adult prostate 10-20% of CaP Benign Prostatic Hyperplasia.

E N D
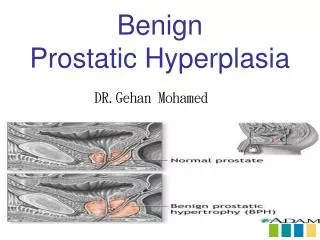
Zonal Anatomy of the Prostate • Peripheral zone • 70% of volume of young adult prostate • 60-70% of CaP • Central zone • 25%: young adult prostate • 5-10% of CaP • Transition zone • 5%: young adult prostate • 10-20% of CaP • Benign Prostatic Hyperplasia
Incidence & Epidemiology • most common benign tumor in men • age related incidence • prevalence • 20% (41–50 y/o) • 50% (51–60y/o) • >90% (>80y/o). • age related symptoms (prostatic obstruction) • age 55 = 25% obstructive voiding symptoms • age 75 = 50% ↓ force & caliber of urinary stream.
Risk factors: • Genetics • ~50% of men < 60 y/o (autosomal dominant) • ↑ relative risk 4x in 1° ♂ relatives • Race • Etiology • multifactorial and endocrine controlled • stromal and epithelial elements hyperplastic nodules • positive correlation between levels of free testosterone and estrogen and the volume of BPH
Pathology • hyperplastic process ↑ in cell number (cont.) • Microscopic evaluation: nodular growth pattern that is composed of varying amounts of: • Stroma • Collagen (non-responsive to either form of medical therapy) • smooth muscle (alpha-blocker therapy) • epithelium (5-alpha-reductase inhibitors) • enlarged BPH nodules compress outer prostate zones = surgical capsule • separates TZ from PZ • cleavage plane for open enucleation of the prostate during open simple prostatectomies performed for BPH.
Pathophysiology • obstructive component of the prostate • mechanical • prostatic enlargement intrusion into the urethral lumen or bladder neck obstruction high bladder outlet resistance • dynamic obstruction • variable symptomatology • prostatic stroma is rich in adrenergic nerve supply • level of autonomic stimulation thus sets a tone to the prostatic urethra • alpha-blocker therapy ↓ tone ↓ outlet resistance. • secondary response of the bladder to the outlet resistance • irritative voiding complaints • Bladder outlet obstruction detrusor muscle hypertrophy and hyperplasia; collagen deposition mucosal herniation bet. Detrusor muscle bundles FALSE DIVERTICULA (mucosa and serosa only) • Cystoscopic examination: trabeculation (thickened detrusor muscle bundles)
Clinical Findings • Symptoms: • Obstructive • Hesistancy • ↓ force and caliber of stream • Sensation of incomplete bladder emptying • Double voiding • Straining to urinate • Post-void dribbling • Irritative • Frequency • Urgency • Nocturia • AUA Symptom Score questionnaire • Single most important tool used in the evaluation of patients with BPH • recommended for all patients before the initiation of therapy
7 items that ask patients to quantify the severity of their obstructive or irritative complaints on a scale of 0–5 0-7: mild 8-19: moderate 20-35: severe
Signs: • PE, DRE and neurologic exam • Smooth, firm, elastic enlargement of the prostate • Induration: possibility of cancer • Lab Findings: • Urinalysis • Exclude infection/hematuria • Serum creatinine • Assess renal function • Serum PSA (optional)
Imaging: • Intravenous pyelogram or renal US • only in the presence of concomitant urinary tract disease or complications from BPH(hematuria,UTI) • Cystoscopy (not recommended) • may assist in choosing the surgical approach in patients opting for invasive therapy • Cystometrograms and urodynamic profiles • patients with suspected neurologic disease or those who have failed prostate suregery
Differential Diagnosis • urethral stricture, bladder neck contracture • Hx of previous urethral instrumentation, urethritis, or trauma • bladder stone • Hematuria and pain • CaP • DRE abnormalities or an elevated PSA • UTI • Mimic irritativesx of BPH • Urinalysis • Can be a complication of BPH • bladder carcinoma • irritative voiding complaints • urinalysis: hematuria • Neurogenic bladder d/o • hxof neurologic disease, stroke, DM, or back injury • ↓ perinealor LE sensation or alterations in rectal sphincter tone or the bulbocavernosus reflex.
Treatment • A. Watchful Waiting • With mild symptoms (0-7) • Optional: moderate/severe symptoms • B. Medical Therapy • C. Conventional Surgical Therapy • D. Minimally Invasive Therapy
Absolute surgical indications • refractory urinary retention (failing at least one attempt at catheter removal) • recurrent UTI from BPH • recurrent gross hematuria from BPH • bladder stones from BPH • renal insufficiency from BPH • large bladder diverticula
Medical Therapy • Alpha-blockers • contractile properties of the prostate and bladder neck mediated primarily by the subtype alpha-1areceptors • 5-Alpha-reductase inhibitors • Blocks testosterone dihydrotestosterone • Epithelial component; ↓ size of gland and improvement of sx • 6 months of tx
Medical Therapy • Combination Therapy • Doxasozin + Finasteride • Patients most likely to benefit : those with larger glands and higher PSA values • Phytotherapy • Use of plants or plant extracts for medicinal purposes • saw palmetto berry, (Serenoarepens) , the bark of Pygeumafricanum, the roots of Echinacea purpurea and Hypoxisrooperi, pollen extract, leaves of the trembling poplar. • S. repens: most well-studied agent usually at 320 mg/day.
Conventional Surgical Therapy • Transurethral resection of prostate (TURP) • Risks : retrograde ejaculation (75%), impotence (5–10%), and incontinence (<1%) • Complications: bleeding, urethral stricture or bladder neck contracture, perforation of the prostate capsule with extravasation • TUR syndrome: hypervolemic, hyponatremic state due to absorption of the hypotonic irrigating solution • Transurethral incision of the prostate • moderate to severe symptoms and a small prostate often have posterior commissure hyperplasia (elevated bladder neck) • More rapid and less morbid than TURP • two incisions using the Collins knife at the 5- and 7-o’clock positions. The incisions are started just distal to the ureteral orifices and are extended outward to the verumontanum
Conventional Surgical Therapy • Open Simple Prostatectomy • When prostate is too large to be removed endoscopically: open enucleation (glands >100 g) • Open prostatectomy: concomitant bladder diverticulum or a bladder stone is present or if dorsal lithotomy positioning is notpossible • Simple suprapubic prostatectomy • Transvesically • Operation of choice in dealing with concomitant bladder pathology • Simple retropubic prostatectomy • the bladder is not entered • A transverse incision is made in the surgical capsule of the prostate, and the adenoma is enucleated
Minimally Invasive Therapy • Laser Therapy • Two main energy sources of lasers have been utilized—Nd:YAGand holmium:YAG. • coagulation necrosis techniques: Transurethral laser-induced prostatectomy (TULIP) with TRUS guidance. • Visual contact ablative techniques: more time-consuming procedures because the fiber is placed in direct contact with the prostate tissue, which is vaporized
Minimally Invasive Therapy • Interstitial laser therapy places fibers directly into the prostate, usually under cystoscopic control; • may result in fewer irritativevoidingsymptoms, because the urethral mucosa is spared and prostate tissue is resorbed by the body rather than sloughed • Advantages of laser surgery : • minimal blood loss • rare instances of TUR syndrome • ability to treat patients receiving anticoagulation therapy • ability to be done as an outpatient procedure. • Disadvantages • lack of availability of tissue for pathologic examination • longer postoperative catheterization time • more irritative voiding complaints • High cost of laser fibers and generators.
Minimally Invasive Therapy • Transurethral electrovaporization of the prostate • uses the standard resectoscopebut replaces a conventional loop with a variation of a grooved rollerball. • High current densities cause heat vaporization of tissue, resulting in a cavity in the prostatic urethra. • Hyperthermia • Microwave hyperthermia is most commonly delivered with a transurethral catheter. • Transurethral needle ablation of the prostate • uses a specially designed urethral catheter that is passed into the urethra. • Interstitial radio frequency needles are then deployed from the tip of the catheter, piercing the mucosa of the prostatic urethra • High-intensity focused ultrasound • Intraurethralstents • keep the prostatic urethra patent.
INCIDENCE & EPIDEMIOLOGY • Most common cancer • Second leading cause of cancer death • Risk factors: • age • Under 40: 1:10,000 • 40-59: 1 in 103 • 60-79: 1 in 8 • diet • ↑ (fat, meat) • ↓ (low fat, fish, plant based, lycopene, omega 3 FA, vit. E, selenium) • Family history • Recurrent prostatitis
PATHOLOGY • 95% are Adenocarcinoma • The other 5% • 90%: Transitional Cell Carcinomas’ • The remaining are small cell carcinomas or sarcomas • Cytologic characteristics: hyperchromatic, enlarged nuclei with predominant nucleoli . • Cytoplasm : abundant; N-C ratio not helful in dx
60 to 70% (peripheral) • 10-20% (transition) • 5-10% (central)
BASAL LAYER • ABSENT – prostate CA • PRESENT- Normal glands, BPH, precursor lesions (PIN) • If diagnosis of prostate cancer is in question, HMW keratin immunohistochemical staining is used • Stains basal cells, prostate cancer is negative
Prostatic Intraepithelial Neoplasia and Atypical Small Acinar Proliferation (ASAP) are thought to be precursor lesions • Men found to have these lesions may be at an increased risk for developing prostate cancer
GLEASON GRADING SYSTEM • The Gleason score is obtained by adding the primary and secondary grades together • Gleason Grades ranges from 1 to 5 • Gleason scores range from 2 to 10 • Gleason Score of: • 2-4: Well differentiated • 5-6: Moderately Differentiated • 8-10: Poorly differentiated
GLEASON GRADING SYSTEM The most important difference between Gleason pattern 1 and 2 is the presence or absence of circumscription respectively. The focus of cancer is not circumscribed. The glands are round to oval and uniformly placed. There are no sharply-angulated or distorted glands. Even at low magnification, one can easily appreciate the variation in size, shape, and spacing of glands. Many small glands have occluded or abortive lumens. There is no evidence of glandular fusion.
GLEASON GRADING SYSTEM The glands are fused and there is no intervening stroma. Glandular fusion is a hallmark of Gleason grade 4. Tumor cells are arranged in solid sheets with no attempts at gland formation.
TNM STAGING SYSTEM • Clinical staging system: • DRE and TRUS • NOT biopsy
Clinical Findings • Symptoms • Most early stage CaP are asymptomatic • Presence of symptoms suggests locally advanced or metastatic disease • Obstructive or irritative voiding: local growth of tumor • Bone pain: metastatic disease to the bones • Paresthesias and weakness of the LE: cord compression
Symptoms • Difficulty voiding or urinary retention • Weak or interrupted flow of urine • Frequent urination (especially at night) • Pain or burning during urination. • Increased urinary frequency • Blood in urine • Back pain • Painful ejaculation
Clinical Findings B. Signs (Physical Exam) • Digital Rectal Exam (induration) • regional lymphadenopathy • specific signs of cord compression
Clinical Findings C. Laboratory Findings • Azotemia: bilateral ureteral obstruction (from direct extension into the trigone or from retroperitoneal adenopathy) • Anemia: metastatic disease • Alkaline phosphatase: elevated in bone metastases • Acid phosphatase: disease outside the confines of prostate
Clinical Findings • D. Tumor Markers- Prostate Specific Antigen • PSA velocity • PSA density • Age-adjusted reference ranges for PSA • Racial variations in CaP detection • Molecular forms of PSA
Prostate Specific Antigen • PSA Velocity • Rate of change of serum PSA • Annual PSA velocity 0.75 ng/mL - increase risk of cancer, failure of treatment, and development of metastases • PSA velocity significant only when several PSA assays are carried out by the same lab over a period of at least 18 mos. B. PSA Density • Ratio of PSA to gland volume • Elevated approx. 0.12 ng/mL/g of BPH tissue
Prostate Specific Antigen C. Age-adjusted reference ranges for PSA Rise in PSA with increasing age results from prostate gland growth BPH, higher incidence of subclinical prostatitis, growing prevalence of insignificant prostate cancers
Prostate Specific Antigen D. Racial Variations in CaP detection • African-American: higher baseline, worst outcomes E. Molecular Forms of PSA • 2 forms: free and protein bound • 90%- 1-antitrypsin, others - 2-macroglobulin
Clinical Findings E. Prostate Biopsy Systematic sextant prostate biopsy • Most commonly employed technique used in detecting CaP • Obtained under TRUS guidance (apex, midsection, & the base of each side of the prostate at the midsagittal line halfway between the lateral border & midline of the gland) • To predict extracapsular extension & risk of relapse following radical prostatectomy
Systematic sextant prostate biopsy Indications: • Men over age 40 with elevated PSA • Abnormal digital rectal examination (DRE) • Abnormal ultrasound of the prostate (TRUS) • Urinary symptoms without an obstructive etiology of symptoms
Clinical Findings F. Combined Modality Risk Assessment
Imaging 1. TRUS • Useful in performing prostatic biopsies • Providing local staging information if cancer is detected • Allows uniform spatial separation & sampling of the regions of the prostate & also makes lesion-directed biopsies possible • CaP appears as a hypoechoic lesion in the peripheral zone • Provides more accurate local staging than does DRE
TRUS Sonographiccriteria for extracapsular extension: • Bulging of the prostate contour or • Angulated appearance of the lateral margin Sonographic criteria for seminal vesicle invasion: • Posterior bulge at the base of the seminal vesicle • Asymmetry in echogenicity of the seminal vesicle associated w/ hypoechoic areas at the base of the prostate
TRUS Axial transrectalultrasonographic (TRUS) scan shows extensive hypoechoic area (arrows) in the right peripheral zone.
TRUS • Enables measurement of the prostate volume (calculation of PSA density) • PSA density = (π/6) X (AP diameter) X (transverse diameter) X sagittal diameter • Cryosurgery & brachytherapy
Imaging 2. Endorectal magnetic resonance imaging (MRI) • staging accuracy: 51 – 92% • high image quality • operator-dependent • expensive
Imaging 3. Axial Imaging (CT,MRI) • Selectively performed to exclude lymph node metastases in high risk patients who are thought to be candidates for definitive local therapy Criteria: • (-) bone scans • T3 cancers or a PSA>20ng/mL • Primary Gleason grade 4 or 5 cancers
Imaging 4. Bone Scan • Can be omitted in patients w/ • Newly diagnosed, • Untreated prostate cancer who are asymptomatic • Have T1 and T2 disease • Serum PSA concentrations < 15 ng/mL
Imaging 5. Antibody Imaging • ProstaScint: mAb to an intracellular component of PSMA • SPECT images obtained 30mins to assess vasculature and at 72-120 hours Recognizes the intracellular domain of PSMA; only soft tissues are imaged and the test may suffer from both false + and -