Download
1 / 21
220 likes | 601 Views

E N D
1: Simultaneous Measurement of Testosterone and Androstenedione in Women with Suspected Androgen Excess Katherine Duxbury
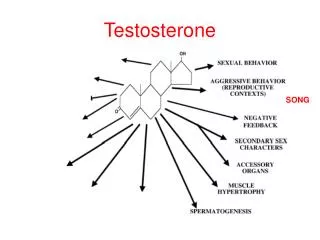
3: Androgens C19 steroid hormones that contribute to the development of secondary sexual characteristics
4: Androgens in Disease Clinical features of hyperandrogenism:
Hirsutism
Acne
Virilisation
5: PCOS Heterogenous syndrome of ovarian dysfunction
Consensus of diagnostic criteria (2 out of 3)
(i) Oligo- or anovulation
(ii) Clinical and/or biochemical signs of hyperandrogenism
(iii) Polycystic ovaries on USS
And exclusion of other aetiologies (CAH, androgen secreting tumours, Cushing�s syndrome)
6: Previous Practice Assessment of androgen status;
7: LC-MS/MS Simultaneous Method
8: Reference Ranges Testosterone 0.27-1.6 nmol/L
9: This Project Aim
Assess the impact of simultaneous measurement
Method
Data collected on 310 female samples
June to October 2005
Testosterone and androstenedione simultaneous measurement
SHBG for FAI calculation
10: Overall Findings
11: Advantages of Simultaneous Measurement Faster service
More evidence for the clinician to more confidently confirm or refute biochemical hyperandrogenism
More information at no extra expense
13: Androstenedione Concentrations
14: Further Investigation
15: Results of Further Investigations
16: Menstrual Cycle Variation
17: Circadian Variation Endocrine Regulations 1998 32 169-176
19: Conclusions The simultaneous measurement of androstenedione and testosterone may offer advantages:
(i) 32% of patients received a faster service
(ii) more evidence at no extra cost
A consequence of simultaneous measurement is the identification of a group of patients with an isolated raised androstenedione.
Obtaining more clinical data about these patients has not yet concluded whether such a result is consistent with PCOS.
20: Further Work Continue requesting extra clinical details for patients with isolated raised androstenedione levels as they are encountered
Investigate the effects of the menstrual cycle on androstenedione levels
Presenting the data to the endocrinology staff and feeding back to the GPs
21: Acknowledgements GPs
Louise Gallagher
Anne Marie Kelly
Brian Keevil