Download
1 / 26
270 likes | 613 Views
Carbapenem resistant enterobacteriaceae update 2012. Dr.T.V.Rao MD. What are Carbapenem resistant enterobacteriaceae ?. E enterobacteriaceae strains resistant to Carbapenem have emerged in the past decade Wide-spread outbreaks have been reported in recent years No reliable treatment options

E N D
Carbapenem resistant enterobacteriaceae update 2012 Dr.T.V.Rao MD Dr.T.V.Rao MD
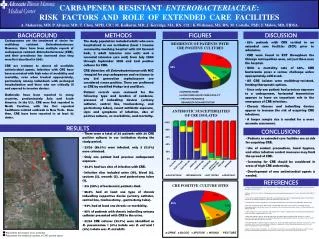
What are Carbapenem resistant enterobacteriaceae ? • Eenterobacteriaceae strains resistant to Carbapenem have emerged in the past decade • Wide-spread outbreaks have been reported in recent years • No reliable treatment options • Huge reservoir of carriers in healthy population • Easy species-to-species spread • Potential devastating health consequences Dr.T.V.Rao MD
Uses by Clinical Syndrome Bacterial meningitis Hospital-associated sinusitis Sepsis of unknown origin Hospital-associated pneumonia How are Carbapenems Used? Use by Clinical Isolate • Acinetobacter spp. • Pseudomonas aeruginosa • Alcaligenes spp. • Enterobacteriaceae • Mogenella spp. • Serratia spp. • Enterobacter spp. • Citrobacter spp. • ESBL or AmpC + E. coli and Klebsiella spp. Reference: Sanford Guide Dr.T.V.Rao MD
Uses by Clinical Syndrome Bacterial meningitis Hospital-associated sinusitis Sepsis of unknown origin Hospital-associated pneumonia How are Carbapenems Used? Use by Clinical Isolate • Acinetobacter spp. • Pseudomonas aeruginosa • Alcaligenes spp. • Enterobacteriaceae • Mogenella spp. • Serratia spp. • Enterobacter spp. • Citrobacter spp. • ESBL or AmpC + E. coli and Klebsiella spp. Reference: Sanford Guide Dr.T.V.Rao MD
Significantly limits treatment options for life-threatening infections No new drugs for gram-negative bacilli Emerging resistance mechanisms, carbapenemases are mobile, Detection of carbapenemases and implementation of infection control practices are necessary to limit spread Emerging Carbapenem Resistance in Gram-Negative Bacilli Dr.T.V.Rao MD
Defining Carbapenem resistance • Definitions for CRE are complicated by a number of factors including the diversity of the genera. Another important challenge to developing a standardized definition of CRE is a recent (mid-2010) change in the Clinical and Laboratory Standards Institute (CLSI) interpretative criteria (breakpoints) for determining susceptibility to Carbapenems among Enterobacteriaceae. Dr.T.V.Rao MD
KPC’s in Enterobacteriaceae Pseudomonas aeruginosa – Columbia & Puerto Rico
Surveillance definition - CDC • CDC has developed the following interim surveillance definition for CRE. CRE are defined as Enterobacteriaceae that are: Nonsusceptible to one of the following Carbapenems: doripenem, meropenem, or imipenem AND Resistant to all of the following third-generation cephalosporin that were tested: ceftriaxone, cefotaxime, and ceftazidime. (Note: All three of these antimicrobials are recommended as part of the primary or secondary susceptibility panels for Enterobacteriaceae) Dr.T.V.Rao MD
KPC Enzymes • Located on plasmids; conjugative and nonconjugativeblaKPC is usually flanked by transposon sequences • blaKPC reported on plasmids with: • Normal spectrum b-lactamases • Extended spectrum b-lactamases • Aminoglycoside resistance Dr.T.V.Rao MD
Changing breakpoints – no need for Hodge test • These new recommendations lowered the breakpoints and removed the requirement for testing for carbapenemases (e.g., modified Hodge Test) to determine susceptibility. Dr.T.V.Rao MD
CRE are epidemiologically important for several reasons: • CRE have been associated with high mortality rates (up to 40 to 50% in some studies). In addition to β-lactam/Carbapenem resistance, CRE often carry genes that confer high levels of resistance to many other antimicrobials, often leaving very limited therapeutic options. “Pan-resistant” KPC-producing strains have been reported. • CRE have spread throughout many parts of the United States and have the potential to spread more widely. Dr.T.V.Rao MD
Screening for CRe • Screening is used to identify unrecognized CRE colonization among epidemiologically-linked contacts of known CRE colonized or infected patients as clinical cultures will usually identify only a fraction of all patients with CRE. Generally, this screening has involved stool, rectal, or peri-rectal cultures and sometimes cultures of wounds or urine (if a urinary catheter is present). Dr.T.V.Rao MD
A new carbapenemases • New Delhi metallo-b-lactamase (NDM-1) • class B b-lactamase • plasmid carrying encoding gene blaNDM • first detected in 2009 from an isolate of K. pneumoniae • Swedish patient with antibiotic-resistant infection acquired and unsuccessfully treated in New Delhi, India • novel gene identified in Sweden Dr.T.V.Rao MD
A new carbapenemases 14 out of 24 patients come from ICU “New Delhi Metallo-β lactamase (NDM-1) in Enterobacteriaceae: Treatment options with Carbapenems Compromised”. Journal of Association of Physicians of India 58: 147–150, March 2010 Dr.T.V.Rao MD • New Delhi metallo-b-lactamase (NDM-1) • over a 3-month period in Mumbai, India, 24 cases of carbapenam resistant isolates were identified • 22 carry the NDM-1 gene • K. pneumoniae (10) • E. coli (9) • 14 samples from ICU • Carbapenem-resistance 0% 8% in 3 years
Some isolates are inherently resistant to Imipenem • For bacteria that have intrinsic imipenem nonsusceptibility (i.e., Morganella morganii, Proteus spp., Providencia spp.), requiring nonsusceptibility to Carbapenems other than imipenem as part of the definition might increase specificity. Dr.T.V.Rao MD
Screening for Carbapenem resistant Enterobacteriaceae • Screening is used to identify unrecognized CRE colonization among epidemiologically-linked contacts of known CRE colonized or infected patients as clinical cultures will usually identify only a fraction of all patients with CRE. Generally, this screening has involved stool, rectal, or peri-rectal cultures and sometimes cultures of wounds or urine Dr.T.V.Rao MD
Previous Breakpoints (M100-S19)MIC (μg/mL) Dr.T.V.Rao MD
Current Breakpoints (M100-S22)MIC (μg/mL) Dr.T.V.Rao MD
Tigecycline: Test by Etest if possible – disk diffusion tends to overcall resistance No CLSI breakpoint, but there are FDA breakpoint Susceptible ≤ 2 mg/ml Intermediate = 4 mg/ml Resistant ≥ 8 mg/ml Testing Other Drugs Dr.T.V.Rao MD
Polymyxin B or Colistin Could test either, but colistin used clinically Disk diffusion test does not work – don’t use! Etest – works well, but not FDA cleared Broth micro dilution – reference labs Breakpoints - none MIC ≤ 2 mg/ml, normal MIC range MIC ≥ 4 mg/ml indicates increased resistance Testing Other Drugs Dr.T.V.Rao MD
Surveillance • Inpatient facilities should have an awareness of whether or not CRE (at least E. coli and Klebsiella spp.) have ever been cultured from patients admitted to their facility and, if so, whether these positive cultures were collected within 48 hours of admission. • If CRE have been present, facilities should also determine: If there is evidence of intra-facility transmission Which wards/units are most affected Dr.T.V.Rao MD
What is our role – contain spread • Carbapenem-Resistant Enterobacteriaceae is an emerging threat to hospitalized patients • Global spread • High mortality • Treatment options are limited • Active surveillance should be performed for high risk patients with overseas hospitalization in past 6 months • Contact tracing / screening for confirmed cases • Importance of infection control measures • High vigilance in critically ill ICU patients Dr.T.V.Rao MD
Hand washing still the best option to prevent spread of CRE • Hand hygiene is a primary part of preventing multidrug-resistant organism (MDRO) transmission. Facilities should ensure that healthcare personnel are familiar with proper hand hygiene technique as well as its rationale. Dr.T.V.Rao MD
Programme Created by Dr.T.V.Rao MD for Medical and Paramedical students in the Developing World • Email • doctortvrao@gmail.com Dr.T.V.Rao MD