Download
1 / 57
600 likes | 705 Views
Explore the detailed stages of embryological and fetal development from conception to birth, along with the midwife's role in promoting maternal and fetal well-being. Gain insights into the time scale of development and the adaptation to extrauterine life. Learn about the critical changes in fetal circulation and the transition at birth. This comprehensive guide provides essential information for healthcare professionals and parents alike.

E N D
DR. Areefa Albahri Chapter 7The fetus By DR. Areefa Albahri Assistant Prof. of MCH Islamic University of Gaza
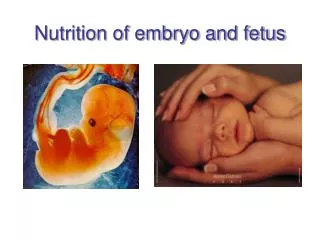
Introduction • The midwife's role in embryological and fetal development is focused on health education for maternal and fetal well-being. This involves providing parents with information about the effects of maternal lifestyle, such as diet, smoking, alcohol, drugs and exercise, on fetal growth and development. Additionally, an understanding of fetal development is of value when a baby is born before term.
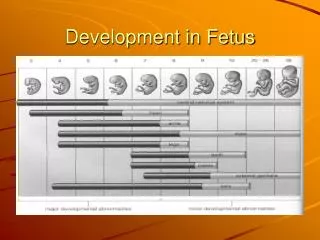
Time scale of development • Embryological development is complex and occurs from weeks 2–8; and includes the development of the zygote in the first 2–3 weeks after fertilization. Fetal development occurs from week 8 until birth. The interval from the beginning of the last menstrual period (LMP) until fertilization is not part of pregnancy. However, this period is important for the calculation of the expected date of birth.
Summary of embryological and fetal development embryo 0–4 weeks •Primitive streak appears Blastocyct implantation •Primitive central nervous system forms •Heart develops and begins to beat •Covered with a layer of skin •Limb buds form •Gender determined. .
4–8 weeks • • Very rapid cell division • • Blood is pumped around the vessels • • Lower respiratory system begins • • Head and facial features develop • • Early movements • • Visible on ultrasound from 6 weeks.
Fetus • 8–12 weeks • • Rapid weight gain • • Eyelids fuse • • Urine passed • • Swallowing begins • • External genitalia present but-gender not distinguishable • • Fingernails develop • • Some primitive reflexes present.
12–16 weeks • • Rapid skeletal development • lanugo appear • • Meconium present in gut • • Nasal septum and palate fuse • • Gender distinguishable. • Able to suck
16–20 weeks • • Constant weight gain • • ‘Quickening’ • • Fetal heart heard on auscultation • • Vernix caseosa appears • • Skin cells begin to be renewed.
20–24 weeks • • Most organs functioning well • • Eyes complete • • Periods of sleep and activity • • Ear apparatus developing • • Responds to sound • • Skin red and wrinkled.
28–32 weeks • Begins to store fat and iron • Testes descend into scrotum • Lanugo disappear from face • Skin becomes paler and less wrinkled. • 24–28 weeks • survival may be expected if born • Eyelids open • Respiratory movements.
32–36 weeks • Weight gain 25 g/day • Increased fat makes the body more rounded • Lanugo disappears from body • Nails reach tips of fingers • Ear cartilage soft • Plantar creases visible.
36 weeks–Birth • •Birth is expected • •Shape rounded • •Skull formed but soft and pliable.
The fetal circulation • The placenta is the source of oxygenation, nutrition and elimination of waste for the fetus. • The ductus venosuswhich connects the umbilical vein to the inferior vena cava • The foramen ovalewhich is an opening between the right and left atria • The ductus arteriosuswhich leads from the pulmonary artery to the descending aorta • The hypogastric arterieswhich branch off from the internal iliac arteries and become the umbilical arteries when they enter the umbilical cord.
The fetal circulation takes the following course: • Oxygenated blood from the placenta travels to the fetus in the umbilical vein. The umbilical veins divide into the portal vein in the liver,& the ductus venosus joining the inferior vena cava. Most of the oxygenated blood that enters the right atrium passes across the foramen ovale to the left atrium and the left ventricle, and then the aorta. The head and upper extremities receive approximately 50% of this blood via the coronary and carotid arteries, and the subclavian arteries respectively. The rest of the blood travels down the descending aorta. A little blood travels to the lungs in the pulmonary artery, for their development.
Adaptation to extrauterine life • At birth, there is a dramatic alteration to the fetal circulation and an almost immediate change occurs. The cessation of umbilical blood flow causes a cessation of flow in the ductus venosus, a fall in pressure in the right atrium and closure of the foramen ovale. As the baby takes the first breath, the lungs inflate, and there is a rapid fall in pulmonary vascular resistance.
Adaptation to extrauterine life • The ductus arteriosus constricts due to bradykinin released from the lungs on initial inflation. The effect of bradykinin is dependant on the increase in arterial oxygen. In the term baby, the ductus arteriosus closes within the first few days of birth.
These structural changes become permanent and become as follows: • The umbilical vein becomes the ligamentum teres • The ductus venosus becomes the ligamentum venosum • The ductus arteriosus becomes the ligamentum • The foramen ovale becomes the fossa ovalis
The fetal skull • The fetal head is large in relation to the fetal body compared with the adult . Additionally, it is large in comparison with the maternal pelvis and is the largest part of the fetal body to be born.
Divisions of the fetal skull • The skull is divided into the vault, the base and the face. The base comprises bones that are firmly united to protect the vital centres in the medulla. The face is composed of 14 small bones which are also firmly united and non-compressible. The vault is the large, dome-shaped part above an imaginary line drawn between the orbital ridges and the nape of the neck.
The bones of the vault • The occipital bone lies at the back of the head. Part of it contributes to the base of the skull as it contains the foramen magnum, which protects the spinal cord as it leaves the skull. The ossification centre is the occipital protuberance. • The two parietal bones lie on either side of the skull. The ossification centre of each is called the parietal eminence.
The two frontal bones form the forehead or sinciput. The ossification centre of each is the frontal eminence. The frontal bones fuse into a single bone by 8 years of age. • •The upper part of the temporal bone on both sides of the head forms part of the vault.
1. SOB, 9.5 2. SOF 10.0 3. OF, 11.5 4. MV, 13.5 5. SMV,11.5 6. SMB, 9.5
SOB, sub-occipitobregmatic 9.5 • SOF, sub-occipitofrontal 10.0 • OF, occipitofrontal 11.5 • MV, mentovertical 13.5 • SMV, sub-mentovertical 11.5 • SMB, sub-mentobregmatic 9.5
The longitudinal diameters are: • The sub-occipitobregmatic (SOB) diameter (9.5 cm) measured from below the occipital protuberance to the centre of the anterior fontanelle or bregma
The sub-occipitofrontal (SOF) diameter (10 cm) measured from below the occipital protuberance to the centre of the frontal suture • The occipitofrontal (OF) diameter (11.5 cm) measured from the occipital protuberance to the glabella
The mentovertical (MV) diameter (13.5 cm) measured from the point of the chin to the highest point on the vertex, slightly nearer to the posterior than to the anterior fontanelle • The sub-mentovertical (SMV) diameter (11.5 cm) measured from the point where the chin joins the neck to the highest point on the vertex • The sub-mentobregmatic (SMB) diameter (9.5 cm) measured from the point where the chin joins the neck to the centre of the bregm
Presenting diameters • Presenting diameters • Some presenting diameters are more favourable than others for easy passage through the pelvis and this will depend on the attitude of the head. This term attitude is used to describe the degree of flexion or extension of the head on the neck. The attitude of the head determines which diameters will present in labour and therefore influences the outcome. • There are always two, a longitudinal diameter and a transverse diameter. The presenting diameters determine the presentation of the fetal head, for which there are three:
Cephalic presentation come in three ways • Vertex presentation. When the head is well flexed the sub-occipitobregmatic diameter (9.5 cm) and the biparietal diameter (9.5 cm) present . As these two diameters are the same length the presenting area is circular, which is the most favourable shape for dilating the cervix and birth of the head. The diameter that distends the vaginal orifice is the sub-occipitofrontal diameter (10 cm). • When the head is deflexed, the presenting diameters are the occipitofrontal (11.5 cm) and the biparietal (9.5 cm). This situation often arises when the occiput is in a posterior position.
Face presentation. When the head is completely extended the presenting diameters are the sub-mentobregmatic (9.5 cm) . • The sub-mentovertical diameter (11.5 cm) will distend the vaginal orifice. • Brow presentation. When the head is partially extended and the mentovertical diameter (13.5 cm) and the bitemporal diameter (8.2 cm) present. If this presentation persists, vaginal birth is unlikely.