Download
1 / 28
280 likes | 612 Views
. ID/CC:The patient is an 85 year-old man with asthma who presents to Chest Clinic with worsening cough and wheezing.HPI: The patient describes years of asthma that has been well controlled with ICS and rare albuterol MDI use. 3-4 months ago, he noticed increasing wheezing and dry cough. His exerc

E N D
1. An 85 year-old man with �steroid-resistant� asthma Douglas B. White, MD
February 11, 2002
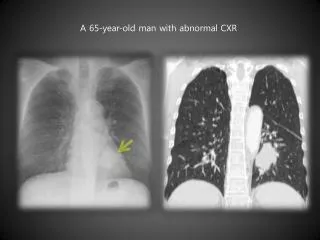
2. ID/CC:The patient is an 85 year-old man with asthma who presents to Chest Clinic with worsening cough and wheezing.
HPI: The patient describes years of asthma that has been well controlled with ICS and rare albuterol MDI use. 3-4 months ago, he noticed increasing wheezing and dry cough. His exercise tolerance decreased and, despite increased ICS, his wheezing worsened. He was treated with multiple steroid tapers with no improvement in his symptoms.
3. HPI (cont)
He presents to clinic with these complaints. He also notes intermittent nausea, abdominal pain and generalized pruritis. He denies fever, chills and myalgias.
4. PMH:
Asthma
Iron Deficiency Anemia
Hyperlipidemia
Gastritis
MEDICATIONS
Fluticasone
Salmeterol
Albuterol MDI
Prednisone 5 mg qod
Rabeprazole
FESO4
5. Social History
20 pk/yr tobacco; quit 1954
No EtOH/drugs
Lives in East Bay with wife
No pets
Ex chef and current dance instructor
POW in Japan & Midway Island during WWII
6. Physical Examination 37.7 140/85 90 12 95% RA
Thin elderly man, NAD
HEENT normal
Lungs: diffuse wheezes and prolonged exp.
CV: normal
Abdomen: scaphoid, soft, NT, ND
Ext: No edema, no rash
7. Labs & Studies WBC: 6.5
PMNs: 3.5
Lymph: 2.7
Eos: 0.79
Hct: 32; MCV: 74
Lytes, Bun, Cr normal
LFTs, coags normal
ESR: 61 Spirometry:
6 weeks ago:
FEV1: 1.7
FVC: 2.5
Current:
FEV1: 1.2
FVC: 2.0
11. Additional Studies HP panel: neg
Sputum: fungal, AFB, bacterial neg
12. Sputum - S. Stercoralis
13. UpToDate vol 10.3 Strongyloides Stercoralis Unique helminthic parasite that can complete its entire life cycle within humans.
Low-level autoinfection may permit organism to exist in human for decades.
Hyperinfection syndrome can be fatal in at-risk patients.
Populations:
Immigrants from endemic areas (tropical and subtropical)
Residents of southeastern USA, Appalachia
Immunocompromised patients (transplant, chronic steroids)
Patients with occupational exposure (veterans, especially POWs)
14. Strongyloides Life Cycle Infection begins with skin exposure to infectious larval stage (usually soil contaminated with human feces).
Filariform larvae migrate hematogenously to lungs, penetrate alveolar sac, ascend bronchial tree and are swallowed into GI tract.
In GI tract, larva mature into adult form? reproduce ? excreted in feces OR access circulation by penetrating intestinal wall (autoinfection).
15. Strongyloides Life Cycle
16. Global Prevalence of Strongyloides
17. Clinical Manifestations of Strongyloidiasis Most Common: mild, waxing and waning, cutaneous, GI or pulmonary symptoms with eosinophilia.
GI Symptoms: epigastric pain, malabsoption, vomiting, diarrhea, Fe-deficiency anemia
Pulmonary Symptoms:
Dry cough, throat irritation, hemoptysis, wheezing
Asthma that worsens with steroid administration
Chronic infection: episodic fever, pulmonary symptoms, infiltrates & eosinophilia.
Skin Reactions: severe pruritis; larva currens: serpiginous urticarial rash
18. Cutaneous Manifestations of Strongyloides: Larva Currens
19. Murray & Nadel, 3rd edition: 1151 Strongyloides Hyperinfection Syndrome Result of parasitic penetration of intestinal wall and hematogenous dissemination with heavy parasite burden.
Rare in immunocompetent hosts; especially associated with corticosteroid use.
Characterized by high fever, abdominal pain, jaundice, larva currens, eosinophilia, pulmonary infiltrates.
�Piggybacking� of bacteria during parasite translocation can cause meningitis, gram negative bacteremia, pneumonia and lung abscess.
20. South Med J. 1996;89:10-19 Characteristics of Pulmonary Strongyloidiasis 20 consecutive patients w/ Strongyloidiasis and pulmonary symptoms.
75% had blood eosinophilia
95% had pulmonary symptoms (cough, SOB, wheezing, hemoptysis)
90% had pulmonary infiltrates
45% developed ARDS
50% had bacterial PNA (enteric organisms)
15% developed bacterial lung abscess
21. AJRCCM 1995;151:205-209 Pulmonary Fibrosis Associated with Disseminated Strongyloidiasis 68 y.o. Puerto Rican man with COPD developed abdominal pain and bloating.
Stool O&P neg. UA revealed strongyloides.
Resolution of symptoms with Thiabendazole
2 years later, progressive COPD? started on chronic steroids.
6 years later, fibrotic lung disease? respiratory failure? death.
Autopsy: interlobular septal fibrosis, multiple granulomas and many S. stercoralis organisms.
22. J Infect Dis. 1981;144:427 Am J Trop Med Hyg 1995;53:248 Diagnosis of Strongyloides Infection Eosinophilia
Stool ova & parasites: 75% sensitive
String test
ELISA: 82% sensitive; min data on specificity
Disseminated Strongyloides:
Larvae can be found in sputum, BAL, stool, pleural fluid, peritoneal fluid.
23. J Infect Dis 1994;169:1076 Treatment of Strongyloides Infection Thiabendazole 25mg/kg PO bid x 3 days
Ivermectin 200ug/kg/day x 1-2 days
Randomized trial of 53 pts with strongyloides in stool & no evidence of hyperinfection treated with either thiabendazole or ivermectin.
35/35 patients treated with Ivermectin, 18/19 treated with Thiabendazole had negative stool O&P at 3 months and resolution of eosinophilia.
95% reported adverse effects w/ Thiabendazole (AMS, depression, nausea)
24. J Infect Dis 1994;169:1076-79 Mean Absolute Eosinophil Count: Response to Therapy
25. Case Follow-up Nine years later, the patient presents to the VA with worsening asthma, weight loss, severe pruritis and persistent iron deficiency anemia.
28. Case Follow-up Eosinophilia
Stool O&P neg x 3
Sputum 0&P negative
BAL: AFB, fungal, bacterial negative
Cytology negative
BAL: few eosinophils
Transbronchial biopsy: pending
29. References Gann et al. RCT of Thiabendazole vs Ivermectin. J Infect Dis. 1994; 169: 1076.
UpToDate 10.3. Strongyloidiasis.
Woodring et al. Clinical & imaging features of pulmonary strongyloidiasis. South med J; 1996;89:10-19
Upadhyay et al. Pulmonary hyperinfection syndrome with S. stercoralis. Am J Med. 2001;110: 167-69.
Lin et al. ILD associated with disseminated S. stercoralis. AJRCCM. 1995; 151:205-09.