Download
1 / 21
311 likes | 663 Views
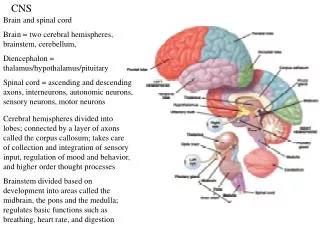
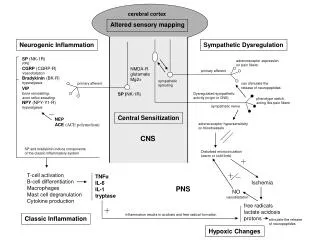
Enhancing Lesions in the CNS. Aaron Grossberg 2012. Increased blood flow Intravascular Rapidly appears after contrast administration. Capillary leak Extravascular /interstitial BBB normally impermeable to contrast Slow appearing Often 10-15 min after administration.

E N D
Enhancing Lesions in the CNS Aaron Grossberg 2012
Increased blood flow Intravascular Rapidly appears after contrast administration Capillary leak Extravascular/interstitial BBB normally impermeable to contrast Slow appearing Often 10-15 min after administration What is contrast enhancement?
Increased blood flow Neovascularity Tumor Granulation tissue capsule Inflammation Reperfusion (post-ischemia) Capillary leak Inflammation Trauma Post surgical changes Granulomatous disease Ischemia Multiple sclerosis What causes contrast enhancement?
Herpes simplex encephalitis extravascular/capillary leak = inflammation Follows olfactory pathways from nasal cavity to brain Medial temporal lobe Uncus Cingulategyrus Cortical Gyral Enhancement Gadolinium – enhanced T1 Smirniotopolous et al. Radiographics. 2009
2. Cerebral infarction (acute) extravascular/capillary leak = endothelial damage Increased blood flow Hyperemia 2º to elevated CO2 after tissue injury Wedge-shaped Cortical Gyral Enhancement CT + contrast Smirniotopolous et al. Radiographics. 2009
3. Cerebral infarction (several weeks later) Vascular hypertrophy = Increased blood flow Fades by 4 weeks – 4 months after event Necessary to repair/remove necrotic tissue Only in reperfused tissue Cortical Gyral Enhancement 4+ weeks Smirniotopolous et al. Radiographics. 2009
Metastatic malignancies Well-circumscribed < 2 cm in diameter Grey matter-white matter junction – most common Primary tumors usually deeper Usually cause symptoms, even when small Due to location of lesions Cortical and Subcortical Nodules CT scan metastatic melanoma Gadolinium-enhanced T1-weighted MR metastatic breast cancer Smirniotopolous et al. Radiographics. 2009
Enhancing Ring hyperemia - inflammation neovascularity - tumor capillary leak - inflammation ** can be due to any ring-enhancing process Center hypoattenuating - necrosis (tumor/abscess) - pus (abscess) - fluid (low grade tumor/cyst) isoattenuating - normal tissue (demyelinating disease) Ring-enhancing lesions Gadolinium-enhanced T1-weighted MR metastatic breast cancer - subcortical/cortical - well-circumscribed - small ( < 2 cm) Smirniotopolous et al. Radiographics. 2009
Enhancing Ring (T1-weighted MRI) neovascular thick - wall > 10 mm irregular Necrotic Center (T1-weighted MRI) Crown of vasogenic edema (T2-weighted MRI) Mass effect High Grade Glioma Gadolinium-enhanced T2-weighted MR Gadolinium-enhanced T1-weighted MR Smirniotopolous et al. Radiographics. 2009
Low Grade Neoplasm Enhancing Ring (T1-weighted MRI) thinner than high grade may appear incomplete - part of ring is neoplastic, part is gliotic (non-enhancing) mural nodule “Cystic” fluid-filled Center (T1-weighted MRI) - not true cyst -“cyst” w/ nodule appearance DDx: Pilocyticastrocytoma (cerebellum) Hemangioblastoma (cerebellum) Ganglioglioma Pleomorphicxanthoastrocytoma Mural nodule Non-enhanced T1-weighted MR Gadolinium-enhanced T1-weighted MR Smirniotopolous et al. Radiographics. 2009
Abscess/Cerebritis includes toxoplasmosis Enhancing Ring (contrast T1-weighted MRI) thin-walled (< 10 mm) – better evaluated on T2-weighted image Non-enhancing Center (contrast T1) - In abscess, center will be hypoattenuated due to pus accumulation - In cerebritis, center may fill in with contrast over 20-40 minutes Perilesional vasogenic edema (contrast T2) Restricted diffusion (diffusion-weighted) - hyperintense Gadolinium-enhanced T2-weighted MR Gadolinium-enhanced T1-weighted MR contrast CT diffusion-weighted MR Smirniotopolous et al. Radiographics. 2009
Demyelination aka multiple sclerosis Enhancing Ring (contrast T1-weighted) faint ring enhancement perivascular, not intravascular often appears “incomplete” Isoattenuated Center (T1-weighted) - no necrosis No perilesional vasogenic edema (T2 –weighted) **If MS is suspected, MRI of spinal cord may show add’l lesions Gadolinium-enhanced T1-weighted MR T2-weighted MR Smirniotopolous et al. Radiographics. 2009
A very simplified approach to ring-enhancing lesions Enhancing rim complete v. incomplete? complete incomplete Center attenuation hypo v. iso? Thick & irregular rim or thin & smooth rim? thin & smooth thick & irregular iso mural nodule? single deep lesion or multiple superficial? hypo Demyelination (multiple sclerosis) no yes multiple superficial single deep abscess/cerebritis metastatic malignancy cystic neoplasm (low grade glioma) high grade glioma (GBM)
Glioblastoma multiforme abscess thick-walled irregular internal ring necrotic, heterogeneous center thin-walled smooth internal ring homogeneous, hypoattenuating center
Multiple sclerosis pilocytic astrocytoma • incomplete ring • isoattenuating center • No vasogenic edema • complete v. incomplete ring • hypoattenuating, fluid-filled center • mural nodule
Periventricular enhancement THICK PERIVENTRICULAR ENHANCEMENT * Neoplastic primary CNS lymphoma - homogenous “lamb’s wool” on contrast-enhanced imaging high grade glial tumor ¤ metastatic lymphoma often involves cortex or meninges THIN PERIVENTRICULAR ENHANCEMENT thin enhancement (< 2 mm) along ventricle margin * Infectious ependymitis/ventriculitis - often CMV in immunocompromised patients Smirniotopolous et al. Radiographics. 2009
Periventricular enhancement THICK PERIVENTRICULAR ENHANCEMENT Primary CNS lymphoma in adult patient with AIDS THIN PERIVENTRICULAR ENHANCEMENT CMV ependymitis MRI CT Non-enhanced enhanced Gadolinium-enhanced, T1-weighted Smirniotopolous et al. Radiographics. 2009
Extra-axial enhancement (meninges) • Dural vs. Pial • - Dura (pachymeningeal) – along surface of skull • - Pia (leptomeningeal)– follows sulci & subarachnoid spaces • Linear vs. curvilinear • Associated with mass/nodule? Dural • Remember: • Thin Dural enhancement normal on CT • Very vascular • No BBB in dura mater • Dura hypo-intense on T1 • Thin linear enhancement with contrast Pial Smirniotopolous et al. Radiographics. 2009
Dural enhancement Intracranial hypotension - increased fluid shifts - increased venous capacitance Meningioma - enhancing hypervascular tumor - enhancing dural “tail” - vasocongestion - interstitial edema Gadolinium-enhanced T1 Gadolinium-enhanced T1 Smirniotopolous et al. Radiographics. 2009
Pial enhancement (meningitis) Bacterial meningitis - thin, linear enhancement - capillary leak - cytokines & bacterial glycoproteins - Fungal meningits may produce thick, lumpy, or nodular enhancement Gadolinium-enhanced T1 Gadolinium-enhanced T1 Contrast-enhanced CT Carcinomatous meningitis - Spread of tumor through subarachnoid space - May still appear thin and linear - capillary leak - cytokines & tumor products Smirniotopolous et al. Radiographics. 2009
Combined dural/pial enhancement Metastatic dural disease - Enhancement of sulci (pial) and inner margin of skull (dural) - Most commonly secondary to breast or prostate cancer; can be lymphoma, as well - lack of BBB predisposes to metastatic seeding FLAIR Gadolinium-enhanced T1 Also seen in CNS granulomatous disease: Sarcoid TB/fungus Wegener granulomatosis Lueticgummas Rheumatoid nodules **All typically involve basilar meninges, Sparing the convexities Smirniotopolous et al. Radiographics. 2009