Download
1 / 26
260 likes | 467 Views
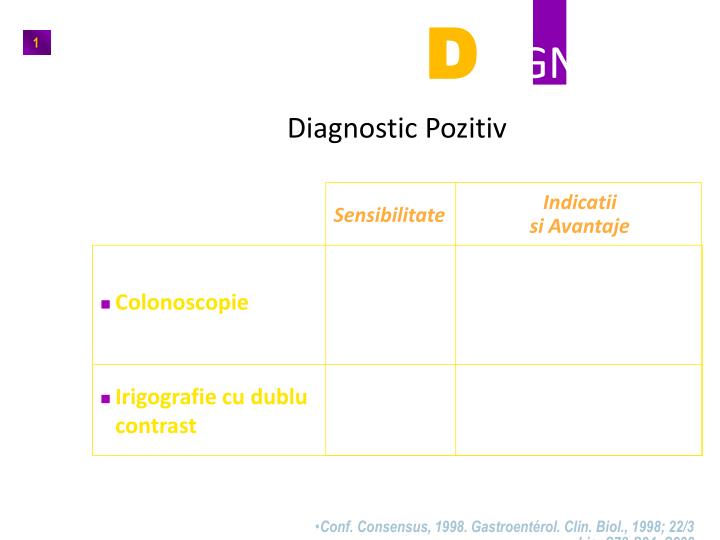
D IAGNOSTIC. 1. Diagnostic Pozitiv. Indicatii si Avantaje. Sensibilitate. - Examen de referinta - diagnostic histologic. Colonoscopie. 96,7%. - Utile(colono este dficila sau contra indicata). Irigografie cu dublu contrast. 84%.

E N D
DIAGNOSTIC 1 Diagnostic Pozitiv Indicatiisi Avantaje Sensibilitate - Examen de referinta - diagnostic histologic • Colonoscopie 96,7% - Utile(colono este dficila sau contra indicata) • Irigografie cu dublu contrast 84% • Conf. Consensus, 1998. Gastroentérol. Clin. Biol., 1998; 22/3 bis: S78-S84; S292
ANATOMIE PATOLOGICA Localizare: 25% colon dr. 15% cec + ascendent 10-18% transvers 18%descendent 35% sigmoid/ rect.
Examen Clinic Semne si simptome generale Tulburari de tranzit intestinal • tendinta la constipatie • tendinta la diaree • alternanta constipatie/diaree Paloare ( anemie feripriva progresiva , fara cauza aparenta ) reducerea apetitului scadere ponderala progresiva – casexie hepatomegalie +/- icter adenopatii periferice
Semne si simptome legate de sediul si marimea tumorii a) colonul drept (asimptomatic): • diaree sau alternanta constipatie/diaree • dureri in flancul/fosa iliaca dreapta • HDI • masa tumorala palpabila (tardiv), sensibila , uneori mobila. b) colonul stang (mai precoce simptomatic) : • Constipatie, sindrom ocluziv intermitent, dureri abdominale, distensie, greata, varsaturi . • scaune cu mucus si sange . c) rect • dureri • rectoragii • tenesme • masa rectala palpabila ( tuseul rectal obligatoriu! ) +/- atingere perineala si pelvina . Afectarea anala se manifesta prin sangerari in afara defecatiei , sange la suprafata scaunului , incontinenta rectala
COMPLICATII Hemoragia digestiva inferioara Ocluzia intestinala Invaginatia Volvulus Peritonita neoplazica Supuratia peritumorala Perforatie Abcese (hepatice, pulmonare, cerebrale) , tromboza venei cave inferioare Fistule MTS : ganglionare, hepatice, peritoneale, pulmonare, pleuro-pulmonare, osoase. Endocardita cu streptococcus bovis
SINDROAME PARANEOPLAZICE ASOCIATE Rare • dermatologice : acanthosis nigricans, dermatomiozita • articulare : osteoartropatie hipertrofica pneumica, artrita reumatoida • vasculare : sdr. Raynaud • neurologice : neuropatii, ataxie • endocrine : sdr. Cushing , hiperparatiroidism
EXTENSIE 8 Sistematic Examen clinic complet antecedente familiale Bilant biologic (hemograma + Bilant hepatic) ACE Colonoscopie completa Echografie abdominala Radiografie pulmonara F + P Optiuni Echo-endoscopie rectala TDM IRM PET • S.O.R. Cancer du côlon, 1995; 99-100.Conf. Consensus, 1998. Gastroentérol. Clin. Biol., 1998; 22/3 bis: S85-S89; S292
9 EXTENSIE • Metastaze Ficat 35% Plamani 19% Retroperitoneu 13% Os 4% Ovare 1-2% Suprarenale 1-2% • S.O.R. Cancer du côlon, 1995; 131.Conf. Consensus, 1998. Gastroentérol. Clin. Biol., 1998; 22/3 bis: S168-S176.
Extensie 10 • Meta pulmonare
A B1 B2 C1 C2 EPITELIU MUCOASA MUSCULARIS MUCOSAE SUB-MUCOASA MUSCULARA LIMITA EXTERNAPERETE SUB-SEROASA SEROASA GANGLIONI (N) + + FACTORI PROGNOSTICI 11 • Cancer Colorectal : Clasificarea Astler-Coller (Dukes modificata) (1) A : Afectare mucoasa si submucoasa B1 : Afectarea muscularei B2 : afectarea muscularei,subseroasa, seroasa C1: B1 si ggl proximali C2 : B2 ggl distali D: Metastaze (1) Astler V.B., Coller F.A. Ann. Surg., 1954; 139: 846-852
Tis T1 T2 T3 T4 Extensie la un organ adiacent FACTORI PROGNOSTICI 12 • Cancer Colorectal : Clasificare TNM (1) T: Tumora primitiva Tis : Carcinom in situ T1: afectare submucoasa T2 : afectarea muscularei T3: subseroasa, seroasa, grasime pericolica T4: afectarea cavitatii peritoneale tanseroasa sau extensie la oraganele vecine prin contiguitate 1. Colon and rectum. In: Hermanek P., Sabin L.H. (eds). TNM classification of malignant tumours (4th ed.) Berlin: Springer - Verlag 1992: 52-55
FACTORI PROGNOSTICI 13 • Corespondenta Clasificarilor STADIU TNM ASTLER COLLER 0 I II III IV Tis T1 T2 T3 T4 T1-T2 T3 T4 Tout T N0 N0 N0 N0 N0 N1-3 N1-3 N1-3 Tout N M0 M0 M0 M0 M0 M0 M0 M0 M1 A B1 B1 B2 B3* C1 C2 C3** D * B3 (Gunderson-Sosin) :tumeur perforant le péritoine viscéral et/ou envahissant les organes de voisinage ** C3 (Gunderson-Sosin) :tumeur perforant le péritoine viscéral et/ou envahissant les organes de voisinage avec envahissement ganglionnaire Monges G. et coll. Lettre Cancérol. Déc. 1996; suppl. : 41-48
FACTORI DE PRONOSTIC 14 • Supravietuire la 5 ani in functie de Stadiu Stadiu T1, N0, M0 T2,N0,M0 T3, N0, M0 T4, N0, M0 Duke ’s A Duke ’s B T3, N0, M0 Supravietuire la 5 ani (%) 97 90 78 63 82 73 80 De Vita.VT 5th Edition Chapter 32.7 p1166
Factorii prognostici majori 15 invazie transparietala invazie organe de vecinatate invazie ganglionara numar de ggl : N > 4* prezenta metastazelor ACE crescut * Trebuie examinati minim 12 ganglioni S.O.R. Cancer du côlon 1995 : 90-91 Conf. de Consensus, 1998, Gastroentérol. Clin. Biol. 1998; 22/3 bis : S115-S125 AJCC Consensus Conf. Cancer 2000; 88 (1) : 1739-57
AltiFactori De PrognosticDefavorabil 16 ocluzie perforatie Aspect infiltrant invazie vasculara venoasa si limfatica invazie peri-nervoasa Grad histologic de diferentiere Tip histologic : forme cu celule in inel cu pecete Numar de ganglioni prelevati < 6 Prezenta unui reliquat tumoral S.O.R. Cancer du côlon 1995: 90-95
Factori Discutabili 17 Sex : prognostic mai favorabil la femei varsta : < 40 ani si > 70-80 ani:prognostic defavorabil Rasa caucaziana: prognostic bun Transfuzii peri-operator Durata simptome inaintea tratamentului colon drept:prognostic mai prost 1. S.O.R. Cancer du côlon 1995: 90-95
FACTORI PROGNOSTICI IN CURSDe EVALUARE 18 Continutul de ADNploidie index de proliferare Citogenetica - anomalii cromosomiale in 70% din cazuri - rearanjari cromosomiale frecvente: 1, 6, 7, 8, 13, 14, 17, 18 Proteine / markeri de suprafata alti factori C-erbB2, timidin fosforilaza, VEGF, metaloproteinazele,densitatea microvaselor S.O.R. Cancer du côlon 1995: 90-95 Conférence de Consensus 1998, Gastroentérol. Clin. Biol. 1998, 22/3 bis: S119-S123 André.T et Callard.P Revue de presse d ’oncologie clinique : 2000 ; 9 ; 3: 18-22
FACTORI PROGNOSTICI IN CURSDE EVALUARE 19 Biologie moleculara Mutatie p53 si K-ras deletie DCC (18q) Thymidylate synthetase (TS) Instabilitatea microsatelitilor (MSI) Genele Nm23A si Nm23B (Non Metastatic clone 23) Fibroza / inflamatie peritumorala Imunohistochimie Hiperexpresie a proteinei p53 Micrometastaze medulare S.O.R. Cancer du côlon 1995: 90-95 Conférence de Consensus 1998, Gastroentérol. Clin. Biol. 1998, 22/3 bis: S119-S123 André.T et Callard.P Revue de presse d ’oncologie clinique : 2000 ; 9 ; 3: 18-22
FACTORI PROGNOSTICI 20 • Pacientii cu metastaze hepatice nerezecate (1) 554 cazuri(1985-1986) Risc relativ de deces • Indicele OMS 2-3 vs 0-1 • Fosfataza alcalina> vs normales • Nr de segmente invadate > 4 vs < 4 • Meta extra-hepatice + vs - • Chimioterapie nu vs da • Colon drept vs rest • PT > 75% vs < 75% • Tumora primara pe loc vs rezecata 1,9 1,6 1,6 1,4 1,4 1,4 1,4 1,2 1. ROUGIER P. and al. FFCD Br. J. Surg. 1995; 82 (10) : 1397-1400
FACTORI PROGNOSTICI 21 • Metastazele hepatice FFCD (1) supravietuire 1 an (%) 47 38 13 Grup 1 2 3 scor OMS 0 0 > 1 > 1 FALC normal anormal normal anormal Supravietuire 2 ani (%) 23 12 1 1. ROUGIER P. and al. (FFCD) Br. J. Surg. 1995; 82 (10) : 1397-1400
Tratament • Chirugical • Laparoscopie • Stapling • Curage ganglionar • Rezectie metastaze • Colostomie • Proteze endoscopice • Radioterapia preoperatorie-rect
Tratament • Chimioterapia • 5FU • Leucovorin • Irinotecan • Oxaliplatin • Cetuximab(EGFR) • Bevacizumab(VEGF)
RECIDIVE 24 • Localizarea primelor recidive dupa chirurgie curativa(1) n = 818 pacienti Dukes B2 ou C - urmarire > 7 ani RECIDIVE (43%) • Af initiala • Colon 40% • Rect 52% • Sediu • Ficat 33% • Plaman 22% • recidiva loc./ reg. 21% • Intra-abdominal 18% • Retro-peritoneal 10% • Adenopatii perif. 4% 1.GALANDIUK S. and al. Surg. Gynecol. Obstet. 1992; 174 (1) : 27-32
Supraveghere Cancer Colo-Rectal Stadiu A sau B1 in primii 5 ani dupa exereza curativa 25 • COLON (1, 3) • Examen clinic la 3 la 3 luni pentru primii 2 ani apoi la 6 luni pentru 3 ani • Colonoscopie la 1 an apoi in functie de rezultate • RECT (2, 3) • Examen clinic la 6 luni pentru 2 ani apoi 1 data pe an • Echoendoscopie rectala • Coloscopie la 1 an • Radio. thorax si echo. Hepatica la 18 luni pentru 3 ani 1. S.O.R. Cancer du côlon 1995 : 131-133 2. S.O.R. Cancer du rectum 1998 : 188-194 3. Conf. Consensus Gastroentérol. Clin. Biol. 1998; 22/3 bis : S155-S167
Supraveghere 26 • cancer rectal B2 sau Cin primii 5 ani dupa exereza curativa (1, 2) • Examen clinic la 3 luni pentru 2 ani apoi la 6 luni Dosaj ACE la 3 luni pentru 2 ani apoi la 6 luni Echografie hepatica la 6 mois pentru 3 ani apoi anual • Echoendoscopie rectala la 3 luni pentru 2 ani apoi anual daca exista anastomoza joasa • Coloscopie la 1 an si apoi in functie de rezultat • Radiografie de torace anual 1. S.O.R. Cancer du rectum 1998 : 188-194 2. Conf. Consensus Gastroentérol. Clin. Biol. 1998; 22/3 bis : S155-S167