Download
1 / 74
1.04k likes | 2.67k Views
Ouchh!. Applied respiratory physiology: part 1. b y; Dr Mohd Ridhwan bin Mohd Noor Intensivist HSNZ 2013. Pre master basic science. Knowledge decay after specialist graduation. Content . Functional anatomy Deadspace / lung volumes/ shunts Ventilation/perfusion abnormalities

E N D
Ouchh! Applied respiratory physiology: part 1 by; DrMohdRidhwan bin Mohd Noor Intensivist HSNZ 2013 Pre master basic science
Content • Functional anatomy • Deadspace/ lung volumes/ shunts • Ventilation/perfusion abnormalities • Control of respiration • Non respiratory functions of lungs
Functional anatomy • Nose, mouth & pharynx humidify & filter the air gases • Larynx is 18 mm in diameter & 11 cm in length • Trachea divides to main stem bronchus at carina (T4) • Bronchi divides 23 times (generations) & the first 16 are termed conducting zone & forms anatomical deadspace • Generation 17-23 where gas exchange occurs with 300 million alveoli & about 2-3 litres in volume
Consists of 3 type of cells; • Type 1 • Provide thin layer of cytoplasm & cover 80% of gas exchange zone • Type 2 • Formation of surfactant & other enzymes • Type 3 • Maintain lungs defense system – alveolar macrophages
Clinical points • ETT should be 1-2 cm above carina or at T3 • Right main bronchus divides from trachea at less acute angle, therefore prone to endobronchial intubation • ® upper lobe bronchus arises few cm from carina, therefore for one lung ventilation (L) double lumen ETT is favored to avoid risk of ® upper lobe collapse with ® double lumen tube
Dead space • Def;lung volume that does not participate in gas exchange (wasted ventilation) or ventilation without perfusion • Types: • Anatomical deadspace • Physiological deadspace • Alveolar deadspace • Apparatus deadspace
Anatomical deadspace • Volume of conducting airways (150 mls in adults) • Mostly atmospheric gas & it’s exhaled gas before CO2 flowing to the alveoli & expired • Influenced by age, position, height, hypoventilation, atropine, hypothermia
Fowler’s methods (anatomical deadspace) • Subject breathing to pneumatachograph & rapid nitrogen analyser • Subject breaths 100% of O2 & N2 concentration plotted against time & volume
Alveolar deadspace • Part of inspired gas that enter the alveoli BUT does not participate in gas exchange • Represents ventilated but underperfused alveoli • Can be measured by comparing PAO2 & PaCO2 • Negligible in healthy adult & PACO2 almost equal PaCO2
Causes ETCO2 < PaCO2 • Low cardiac output or hypotension • High inspiratory pressure esp high PEEP • Pulmonary embolus • Posture changes – leading to changes in regional perfusion
Physiological deadspace • Alveoli + anatomical deadspace • Part of tidal volume not participate in gas exchange • Calculated using Bohr equation; Vd = PaCO2 – PECO2 VtPaCO2 • Normally ~ 30% of tidal volume • Clinical: increase in physiodeadspace cause alveolar ventilation reduced unlesscompensatory increase in minute volume e.g. COPD
Lung volumes SpirometryTacing in adult male
Lung volumes The volume (per kg) The capacities (per kg) Total lung capacity 75-80 mls Vital capacity 60-70 mls Inspiratory capacity 50 mls Funtional residual capacity 30 mls • Residual volume 15-20 mls • Expiratory reserve volume 15 mls • Tidal volume 6-8 mls • Inspiratory reserve volume 45 mls
Which volumes & capacities can’t be measured by spirometry? • Residual volume • Any capacities which contain residual volumes • FRC • Total Lung Capacity (TLC)
Functional residual capacity (FRC) • Def: volume of gas which remains at the end of normal expiration (FRC = RV + ERV) • It is a balance point between tendency of the chest wall to move outward & tendency of the lungs to collapse
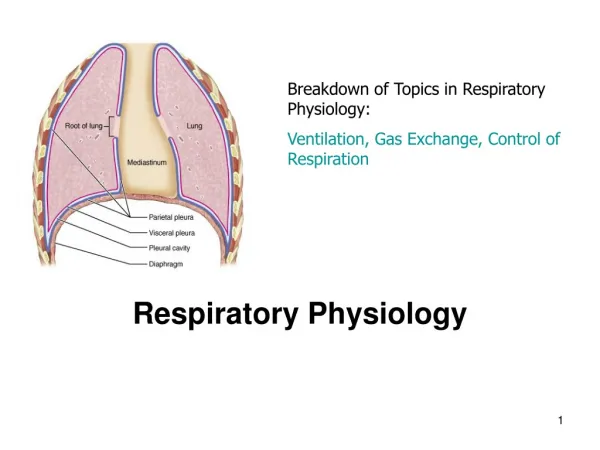
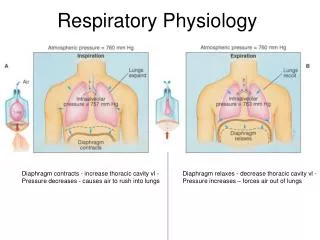
Forces exerted on the thorax The tendency of the chest wall and diaphragm to separate from the lungs is the reason why intrapleural pressure is negative
Functions of FRC • Oxygen store • Buffer to maintain a steady arterial pO2 • Prevent atelectasis • Minimise work of breathing (by keeping the lungs on the steep part of the compliance curve) • Minimise pulmonary vascular resistance • Minimise V/Q mismatch
FRC as oxygen store • At room air PAO2 of 100 mmHg & FRC of 2200 mls, the lungs contain 290 mls of O2. • Pre-oxygenation with 100%, it can increase up to 1800 mls of O2 in the lungs
Buffer for arterial PO2 • Continuous presence of gas containing in the lungs converts the intermittent tidal delivery into continuous availability of O2 for gas exchange. • Prevent large swings in PaO2 during ventilatory cycle
3. Prevent atelectasis • FRC maintain partial state of partial inflation in the lungs & prevent atelectasis • At a balance point between the tendency of the chest wall to move outward & the tendency of the lung to collapse
Minimize work of breathing • At FRC, the lung work at the steep part of compliance curve • Minimise pulmonary vascular resistance • PVR varies with lung volume, high at both high and small lung volume • PVR lowest at FRC
Minimize V/Q mismatch • FRC prevent lung closure at tidal ventilation & minimize ventilation abnormality
Measurement of FRC • Gas dilution methods (nitrogen washout/helium washin) • Subject rebreathing from closed circuit that contain initial volume (V1) & concentration of helium (He1) • After period of rebreathing final helium (He2) measured V1 x (He1) = (V1 + FRC) x (He2)
Factors affecting FRC Increase Decrease Obesity Muscle paralysis Changing from erect to supine Pregnancy Anaesthesia Pulmonary ds causing increased elastic recoil of the lungs • Height • Changing from supine to erect position • Decreased lung elastic recoil (e.g. emphysema) • PEEP
Closing capacity • Lung volume at which airways start to close in expiration ( CC = CV + RV) • Factors increasing CC; • Increasing age • Smoking/asthma/emphysema/bronchitis • Prolonged recumbency • Increase left atrial pressure
Closing volume measurement Single breath Nitrogen washout
Relationship between FRC and closing capacity 66 yrs 44 yrs
Describe West’ zones of the lung • Describe relationships of pulmonary arterial, venous & alveolar pressure in zones from apex to the base • Changes occur due to gravity that cause distension of vessels at the upright lung base & compression at the apex • PAP decrease by 1 cmH2O per cm vertical distance of the lung
At the base PAP 10 cmH2O (16 26) & PVP fr 11-21 cmH2O • At the apex PAP 15 cmH2O (16 1) & venous pressure fr. 11 to -4 cmH20 # need to put head down position to avoid air embolism during CVC insertion#
West’s zones • Zone 1: alveolar pressure exceed arterial pressure. Creating no flow in apex and deadspace # Contribute to deadspace. Rarely occur in healthy subject but in hypotension, hemorrhage or use of PEEP will increase zone 1.#
West’s zones • Zone 2; Pa exceeds PA but PA still above PV on expiration. The flow or perfusion depends on difference ( Pa – PA) & called waterfall effect
West’s zones • Zone 3; Pv more than PA in inspiration & expiration. Flow depend on (Pa –Pv). • Pulmonary blood flow is constant in this region & provide optimal condition for gas exchange #Swan-Ganz should float here posteriorly in supine position#
West’s zone • Zone 4: the lung has positive interstitial pressure (PE, mitral stenosis, pulmonary edema) • Flow depends on difference between Pa and Pi
What the 7 differences between apex and base of lungs? • Alveoli at the top of the lungs; • Larger at end-expiration • Have lower ventilation • Have lower perfusion • Have higher V/Q ratio (3.3 vs 0.63) • Higher pO2 (132 at apex, 89 at base) • Lower pCO2 (28 at apex, 42 at base) • Higher pH (7.51 vs 7.39)
Shunts • True shunts is perfusion without ventilation (V/Q = 0) • Refers to blood that enter arterial system without passing ventilated areas of the lungs • Effects; • Reduce PaO2 • Increase A-a gradient
Venous admixture • Amount of mixed venous blood has to be added to pulmonary end capillary blood to see drop in arterial PaO2 • Sometimes used interchangeably with shunts
2 main sources of blood contribute to venous admixture • True shunts – 2 sources • Bronchial vein • Thebesian vein • Blood from alveoli with V/Q less than 1 e.g. atelectasis, consolidated area, edema
Recollection V/Q = 1 V/Q < 1 V/Q > 1
Shunt equation Flow thro lungs = Qt - Qs Shunted flow = Qs Total flow = Qt Shunt O2 content = CvO2 Total O2 delivery = O2 delivery from ventilated lungs + O2 delivery from shunt
O2 flux/delivery = cardiac output x O2 content Total O2 delivery = O2 delivery from ventilated lungs + O2 delivery from shunt Qt x Ca = (Qt – Qs) x CcO2 + (Qs x CvO2) Qs = (CcO2 – CaO2) Qt (CcO2 – CvO2
Finally what we get….. V/Q = 0 V/Q = ∞
What methods used to measure V/Q inequalities? • A-a oxygen gradient (normal 5-15 mmHg) • Need alveolar gas equation PAO2= FiO2 x (760-47) – (PaCO2/R) R = 0.8 • Increased in V/Q mismatch, shunting, diffusion abnormalities
Measurement V/Q abnormalities (2)…… • Shunt equation • For low V/Q unit • Bohr equation • For high V/Q unit • PaCO2 – ETCO2 difference • ETCO2 normally 2-5 mmHg lower than PaCO2 • Increase in high alveolar deadspace (PE, low cardiac output, venous air embolism)