Download
1 / 23
440 likes | 1.97k Views
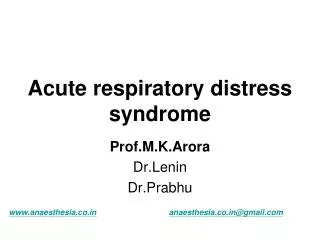
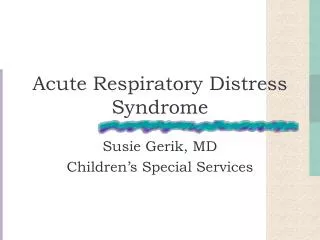
ACUTE RESPIRATORY DISTRESS SYNDROME ( ARDS ). Oea Khairsyaf. Acute Respiratory Distress Syndrome. Defenisi. “Non-cardiogenic Pulmonary Oedema” Ashbaugh, Bigelow et al, 1967 “Adult Respiratory Distress Syndrome” Petty and Ashbaugh, 1971 “Shock Lung” Staub, 1974

E N D
ACUTE RESPIRATORY DISTRESS SYNDROME ( ARDS ) Oea Khairsyaf
Acute Respiratory Distress Syndrome Defenisi • “Non-cardiogenic Pulmonary Oedema” • Ashbaugh, Bigelow et al, 1967 • “Adult Respiratory Distress Syndrome” • Petty and Ashbaugh, 1971 • “Shock Lung” • Staub, 1974 • “Acute Respiratory Distress Syndrome” • American-European Consensus Committee, 1992
Consensus Conference Definitions for Acute Lung Injury (ALI) and Acute Respiratory Distress Syndrome (ARDS)
Asma bronkial PPOK Pneumonia Aspirasi makanan Pulmonary contusion Near-drowning Inhalational injury DLL Sepsis Severe trauma with shock Drug overdose Acute pancreatitis Transfusion of blood products ETIOLOGI ARDS SECARA LANGSUNG TIDAK LANGSUNG
Acute Respiratory Distress Syndrome Gambaranklinis: • Awal “shock” responsifterhadapresusitasi. • Periode latent : beberapa jam, biasanyabeberapahari (12-48 jam). • Insidious tachypnoea, pasienjadigelisah . • Paru tidal volume kecil, napascepat, hipoksemiarefrakter. • Mula-mula alkalosis respiratorik asidosisrespiratorik • Ventilasimekanis
Patogenesis 3 fasedari lung injury: • Faseexudatif ( edema and perdarahan ) • Fase inflammatory and repair • Fase fibrotic
Acute Respiratory Distress Syndrome Exudative Phase, 0-5 hari. • Ruang alveoli terisicairan, protein dan inflammatory cells. • Necrosis sel-selpneumocyte type 1, fibrin, platelet thrombi. Inflammatory Phase, 5-10 hari. • Proliferasi fibroblasts dansel-selpneumocyte type 2. • Squamousmetaplasiadanpembentukan hyaline membranes. Fibroproliferative Phase, 10 harisampaisembuhataumati. • Fibrosis interstitaldan intra-alveolar. • Thrombosis danobliterasivaskuler. • Collagen parumeningkat.
Inflammatory Response Neutrophil activation Neutrophils in BAL Histology appearances ROS Reactive Oxygen Species Superoxide / Hydroxyl Alveolar / capillary permeability Protein levels in BAL Lung Water Pulmonary Oedema ARDS / ALI Pathogenesis ARDS / ALI Precipitating Event
Patogenesis ARDS / ALI REDOX Balance Generation of Oxidant species Antioxidant Protection Superoxide dismutase Catalase Glutathione Transferrin Ceruloplasmin Vit E Vit C Beta-carotene ROS H2O2 Superoxide (O2.-) Hydroxyl radical (OH-) RNS Nitric oxide (NO) Peroxynitrite (ONOO-) Normal
Patogenesis ARDS / ALI Oxidative Stress Depletion of antioxidants ROS formation & Oxidative damage
Predisposition? Inflammatory Response (Respiratory Burst) ROS RNS Molecular Damage and Dysfunction Alveolar / capillary permeability Pulmonary Oedema Ventilatory support Inhaled NO ARDS/ALI The Pathogenesis of ARDS / ALI Precipitating Event Inflammatory mediators signalling Inflammatory mediators
Faktor-faktos seluler dan humoral pada ALI/ARDS • Neutrophils. • ROS dan proteases. • Resting, activated, primed and unresponsive. • Cytokines (polypeptides). • TNF-, macrophages, monocytes, neutrophils. • IL-1, macrophages, endothelial cells • GM-CSF, monocytes, macrophages, fibroblasts epithelial, endothelial dan smooth muscle cells. • Chemokines (chemotactic cytokines). • IL-8. • Eicosanoids (prostaglandin, leucotrienes, thromboxanes), complement, endotoxins, adhesion molecules, PAF, endothelins, NO.
Pathogenesis • Influx cairan edema kaya protein alveoli (permeabilitas alveolar-capillary barrier ) • Kerusakan Type 2 cells gangguan epithelial fluid transport gangguan pengeluaran cairan dan produksi surfactant abnormal • Bila kerusakan hebat gangguan epithelial repair fibrosis • Neutrophils merupakan sel yang dominant • Cytokines dan proinflammatory compounds mengawali dan memperkuat respons inflammatory
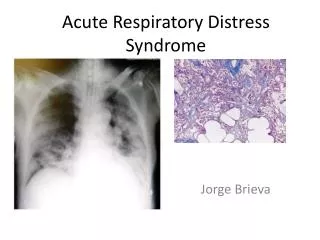
Hyaline membr Collagen Exudative phase (A & D) Fibrosing-alveolitis phase (B, C & E) Ware LB, Matthay MA. N Engl J Med 2000;342:1334-1349
Exudative phase Fibrosing-alveolitis phase Ware LB, Matthay MA. N Engl J Med 2000;342:1334-1349
PENATALAKSANAAN • Obati penyakit dasar • Antibiotika • Kortikosteroid • oksigenasi • Anti oksidan
Keluaran (outcome) • Tahun 1967 - 1979 • Asbaugh (1967) : survival 42% • Survival : 18 – 38% • Tahun 1980 - 1989 • Survival (< 1985) : 32 – 36% • Survival (> 1985) : 41 - 52% (European Collaborative Study 41%) • Tahun 1990 – 2000 • Survival : 41 – 60% • NIH ARDS study : mortality 40% vs 30% (penurunan 25%, antara VT 12 mL/kg vs 6 mL/kg)
Outcome Jangka Panjang pada Survivors (1-1,5 tahun pasca ARDS) Sequelae pulmoner Majoritas, fungsi paru kembali hampir normal Gangguan residual: • restrictive ventilatory defect (biasanya ringan), • Hipertensi pulmoner (ringan), • airflow limitation ( bronchial hyperactivity) Gangguan pada exercise testing lebih bermakna (setara pasien COPD berat) Derajat gangguan ~ umur, riwayat merokok, ventlasi mekanis berkepanjangan
Survival • 10 tahunterakhir, mortalitasturun 20% • Mortalitas: • Umur : 75% (≥ 60 th) vs 37% (< 60 th) • Faktorresiko : 64% (sepsis) vs 42% (trauma) • Penyulit : 86% (sepsis) vs 38% (tanpa sepsis) • Response thd PEEP : PaO2/FiO2 > 150 mmHg mortalitas 23%
TERIMA KASIH TERIMA KASIH