Download
1 / 13
550 likes | 2.56k Views
Approach to Hyponatremia. Core Topic UCI Internal Medicine Residency, 2012. Clinical Scenario. 74-year-old man p/w recent gastroenteritis characterized by n/v/d x 5 days, in addition to fatigue and headache.

E N D
Approach to Hyponatremia Core Topic UCI Internal Medicine Residency, 2012
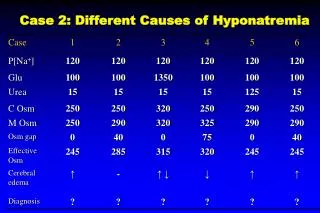
Clinical Scenario • 74-year-old man p/w recent gastroenteritis characterized by n/v/d x 5 days, in addition to fatigue and headache. • CT head (-) in ED. No focal neurologic deficits found. He looks dry on physical exam, with no evidence of fluid overload. • BMP significant for Na+ of 118, baseline unknown. Serum osmolality is 266. Urine osmolality is 377. Urine sodium is 8. • How would you approach this patient’s hyponatremia? • How would your approach be different if this patient presented with new-onset seizures?
Lecture Objectives • Hyponatremia • Clinical manifestations • Diagnostic approach • Clinical Scenario discussed
Hyponatremia Defined • Definition: Serum Na+ <135 meq/L • Generally associated with decreased osmolality to <275 • Most common electrolyte abnormality in the US • Caused by retention of water • Usually a drop in osmolality will suppress ADH to allow excretion of the excess water via dilute urine • Most forms of hyponatremia are associated with elevated ADH (whether appropriate or inappropriate), which concentrates urine
Signs & Symptoms • More profound when the decrease in sodium is very large or occurs rapidly(i.e. over hours) • Generally asymptomatic if Na+ level >125 • Symptoms include: • Headache • Nausea, vomiting • Muscle cramps • Disorientation, depressed reflexes, lethargy, restlessness • Seizure, coma, permanent brain damage, respiratory arrest, brainstem herniation & death • Serious complications are more commonly seen in primary polydipsia, after surgery, and in menstruating women
Approach to Hyponatremia • 1st assess volume status • Is the patient volume overloaded, depleted, or euvolemic? • 2nd assess osmolality (hyper, iso, or hypo) • Is the blood concentrated? For hypotonic hyponatremia, continue to 3rd step: • 3rdassess urinary sodium excretion and FeNa % • Is the urine concentrated? *Remember VOU – volume status, osmolality, and urine studies
STEP 1 – (V) Volume Status • 1st assess volume status (extracellular fluid volume) • Hypotonic hyponatremia has 3 main etiologies: • Hypovolemic – both H2O and Na decreased (H20 < Na) • Consider obvious losses from diarrhea, vomiting, dehydration, malnutrition, etc • Euvolemic – H20 increased and Na stable • Consider siADH, thyroid disease, primary polydipsia • Hypervolemic – H20 increased and Na increased (H2O > Na) • Consider obvious CHF, cirrhosis, renal failure
STEP 2 - (O) Osmolality • 2nd assess osmolality hyper, iso, or hypo • Hypotonic hyponatremia = warrants further workup, especially when there is no obvious fluid overload or depletion • Serum Osmolality: lab value or calculation – in mosm/kg • =(2 x Na+) + (glucose/18) + (BUN/2.8) + (ethanol)/4.6 • Hypertonic - >295 • hyperglycemia, mannitol, glycerol • Isotonic- 280-295 • pseudo-hyponatremia from elevated lipids or protein • Hypotonic - <280 • excess fluid intake, low solute intake, renal disease, siADH, hypothyroidism, adrenal insufficiency, CHF, cirrhosis, etc.
STEP 3 – (U) Urine Studies • For euvolemic hyponatremia, check urine osmolality • Urine osmolality <100 - excess water intake • Primary polydipsia, tap water enemas, post-TURP • Urine osmolality >100 - impaired renal concentration • siADH, hypothyroidism, cortisol deficiency • Check urine sodium & calculate FeNa % • A low urine sodium (<10) and low FeNa (<1%) implies the kidneys are appropriately reabsorbing sodium • A high urine sodium (>20) and high FeNa (>1%) implies the kidneys are not functioning properly
Treatment of Hyponatremia • Be CAUTIOUS with correction: • 0.5 meq/L increase per every hour initially • Do not increase Na more than 10 meq/L in 24 hrs or 18 meq/L in 48 hrs • Treatment varies greatly by etiology of hyponatremia, and it is important to look-up via online or other resources.
Clinical Scenario - Conclusion • 74-year-old man p/w recent gastroenteritis characterized by n/v/d x 5 days, in addition to fatigue and headache. • BMP significant for Na+ of 118, baseline unknown. Serum osmolality is 266. Urine osmolality is 377. • How would you approach this patient’s hyponatremia? The steps: • 1) Serum osmolality – 266, decreased (hypotonic) • 2) Urine osmolality –377, increased (>100) • 3) Volume status - hypovolemic • 4) Urine Na, FeNa – urine Na 8, appropriately reabsorbing, likely volume depleted 2/2 N/V • 5) Treatment: Mild symptoms, correct slowly w/ isotonic saline • How would your approach be different if this patient presented with new-onset seizures? • For symptomatic, severe hyponatremia, more rapid correction using 3% normal saline
TAKE HOME POINTS • Symptoms: Usually Na <125 or rapid decline • N/V, headache, lethargy, AMS, seizures, coma • WORK-UP in 3 important steps (V-O-U): • 1) Assess volume status • 2) Assess serum osmolality • 3) Check urine sodium, osmolarity, & calculate FeNa • Treatment varies by etiology, but cautious correction of sodium important to prevent demyelination as fluid leaves the brain