Download
1 / 51
760 likes | 2.15k Views
Surgical Management of Intra-Articular Distal Humerus Fractures. RP Dunbar IOA-AAOS Program Yogyakarta, Indonesia November 2013. Objectives. Overview of Anatomy Evaluation & Classification Treatment Principles Surgical Steps Outcomes & Pitfalls. Functional Anatomy. Anatomy.

E N D
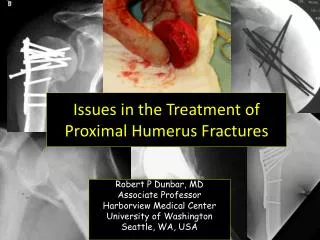
Surgical Management of Intra-Articular Distal Humerus Fractures RP Dunbar IOA-AAOS Program Yogyakarta, Indonesia November 2013
Objectives • Overview of Anatomy • Evaluation & Classification • Treatment Principles • Surgical Steps • Outcomes & Pitfalls
Anatomy • Angulated ant. 15-30° in sagittal plane • 6° valgus of condyles • 3°- 8° internally rotated
Distal humerus strikes proximal ulna Condyles displaced by forearm musculature Mechanism of Injury & Deforming Forces
Distal Humerus/Elbow Anatomy Extra-articular Intra-articular
Three Joints • Ulnohumeral • Radiocapitellar • Proximal Radioulnar
Physical Examination • Open or closed • Neurovascular status • Ulnar n. • Examine shoulder & wrist
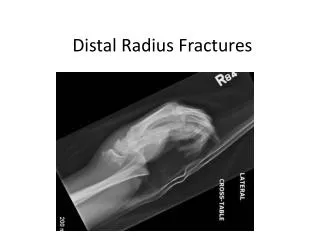
Radiographs AP Lateral Traction View
CT Scan Not Commonly ordered! AXIAL CORONAL REFORMAT
Treatment Goals • Articular Congruity • Anatomic Reduction • Early ROM • Functional Recovery
Preop Planning • Patient Position • Surgical Approach • Olecranon Osteotomy • Triceps Split • Paratricipital • Imaging • Implants
Patient Positioning LATERAL PRONE
Imaging AP Lateral
Approach Radially curved posterior incision Identify/Protect Ulnar Nerve
Olecranon Osteotomy • Intra-articular fractures w/articular comminution • Chevron type osteotomy • Apex distal (bigger piece) • Rotationally stable • Ease of reduction • Consider pre-drilling for later fixation
Olecranon Osteotomy • Oscillating saw: • Cut to level of subchondral bone • Aim for “bare area” • Complete with an osteotome
Coronal Shear Fractures • Can involve capitellum or extend to trochlea • CT scan may be useful • Approach • Lateral vs. osteotomy
Coronal Shear Fracture FixationLag Screws TypicalButtress when Able
Type C FracturesFixation Principles • Fix joint first! • Small articular fragments can be secured with small, countersunk screws • Beware of screw traffic! “Seattle Traffic Jam”
Fixation Principles • Re-attach articular block to diaphysis • Restoring the columns
Fixation Principles • Anatomic fixation of articular segment • Stable fixation of metaphyseal component in anatomic alignment, length, rotation • Important considerations: • Leave fossae unobstructed • Trochlear anatomy/width is critical • Restoration of relationship of columns
Fixation Principles • Anatomic rigid fixation of articular segment • Stable fixation of metaphyseal component in anatomic alignment, length, rotation • Important considerations: • Leave fossae unobstructed • Trochlear anatomy/width is critical • Restoration of relationship of columns
Fixation Principles • Anatomic rigid fixation of articular segment • Stable fixation of metaphyseal component in anatomic alignment, length, rotation • Important considerations: • Leave fossae unobstructed • Trochlear anatomy/width is critical • Restoration of relationship of columns
Fixation Principles • Anatomic rigid fixation of articular segment • Stable fixation of metaphyseal component in anatomic alignment, length, rotation • Important considerations: • Leave fossae unobstructed • Trochlear anatomy/width is critical • Restoration of relationship of columns
Fixation Principles • Anatomic rigid fixation of articular segment • Stable fixation of metaphyseal component in anatomic alignment, length, rotation • Important considerations: • Leave fossae unobstructed • Trochlear anatomy/width is critical • Restoration of relationship of columns
Choice of Implants • Small fragment plates & screws • Pelvic reconstruction plates • Anatomy specific plates (+/- locking capability)
Plate Positioning Lateral-Posterior Medial
TENSION BAND CONSTRUCTS Osteotomy Reduction/Fixation WIRE SCREW
Osteotomy Repair- Plate • Pre-drill intramedullary screw • Compression of osteotomy: • IM screw • Shaft screws
CHECK Range of Motion! NOT DONE YET! • Flexion/Extension • Pronation/Supination • Check for impingement • No crepitus
Ulnar Nerve TranspositionChen et al. JOT 2010 • 48 transposed vs. 89 not transposed at time of ORIF • 33% ulnar neuritis with transposition vs 9% without
Postoperative Care • Bulky splint in extension • +/- drain • Start motion @ 48 hrs • No lifting for 6-8 weeks • +/- Removable splint
Complications • Infection • Stiffness • Heterotopic Ossification • Arthrofibrosis • Arthritis • Loss of Fixation • Hardware Failure • Nonunion
Total Elbow Arthroplasty • Indications: Elderly + Poor bone + Highly comminuted + Low fracture • Unable to obtain goals with ORIF • Stable fixation • Early motion
Summary • Most treated operatively • Olecranon osteotomy when needed • Stable fixation • Protect but don’t tranpose Ulnar n. • Early motion
Extra-articular “A” Fractures • Single plate +/- lag screw • Two plates to support both columns • Relative vs absolute stability