Download
1 / 52
520 likes | 539 Views
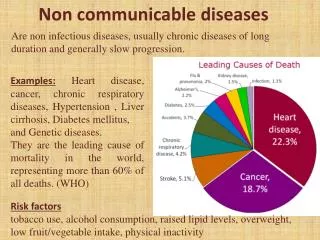
Explore the impact of historical events on health in former Soviet Union countries, focusing on non-communicable diseases and key factors affecting health outcomes, including alcoholism. Analyze the evolution of health care systems and the demographic challenges faced post-Soviet era.

E N D
Non-communicable Diseases and Former Soviet Union countries Eugene Shubnikov, MD, Institute of Internal Medicine, Novosibirsk, Russia
PRESIDENT VLADIMIR PUTINState-of-the-Nation AddressFederal Assembly of the Russian Federation,The Kremlin, April 25, 2005 I am deeply convinced that the success of our policy in all spheres of life is closelylinked to the solution of our most acute demographic problems. We cannot reconcileourselves to the fact that the life expectancy of Russian women is nearly 10 yearsand of men nearly 16 years shorter than in Western Europe. Many of the currentmortality factors can be remedied, and without particular expense. In Russia nearly100 people a day die in road accidents. The reasons are well known. And weshould implement a whole range of measures to overcome this dreadful situation. I would like to dwell on another subject which is difficult for our societytheconsequencesof alcoholism and drug addiction. Every year in Russia, about 40,000people die from alcohol poisoning alone, caused first of all by alcohol substitutes. Mainly they are young men, breadwinners. However, this problem cannot be resolved through prohibition. Our work must result in the young generationrecognizingthe need for a healthy lifestyle and physical exercise. Each young personmust realize that a healthy lifestyle means success, his or her personal success.
Health status • It is useful to begin an account of health status developments with a consideration of the Soviet period, as the present health crisis of the Russian Federation has its roots in events that long precede the collapse of the Soviet Union.
The health care principles upon which the Soviet health care system was to be based (Nikolai Semashko): • Government responsibility for health • Universal access to free services • A preventive approach to “social diseases” • Quality professional care • A close relation between science and medical practice • Continuity of care between health promotion, treatment and rehabilitation.
Next steps following the establishment of the “Semashko” model in 1918 • Russia made massive strides in arresting the spread of infectious diseases. • Drastic epidemic control measures were implemented, particularly in the cases of tuberculosis, typhoid fever, typhus, malaria and cholera. • These involved community prevention approaches, routine check-ups, improvements in urban sanitation and hygiene, quarantines, etc.
Why? • The diverging paths of Russia and other industrialized nations with respect to health status from the 1960s onward has been attributed to the failure of the Russian health care system to successfully respond to the epidemiological transition.
Why? (cont.) • The paternalistic Soviet philosophy did not encourage the development of responsibility of the individual with respect to lifestyle issues that have a major bearing on health (alcohol use, smoking, diet, etc.), a situation exacerbated by the heavy dependence on alcohol sales as a means of circulating currency in a country with little access to consumer goods. And Soviet medical science was effectively isolated from developments in the West, not only in terms of knowledge of new treatments but also access to pharmaceuticals, technology, and the emerging evidence based medicine movement.
A campaign against alcohol • By the 1980s, the gap between Russia and Western countries in life expectancy at birth came to about 10 years for men and 6 years for women, mostly due to high death rates among those of working age (6). In the mid-1980s, the government made an attempt to address this problem (9). It was by then generally understood that potentially avoidable human losses were mostly attributable to excess adult age mortality from particular causes such as injuries, accidental poisoning, suicide, homicide, sudden cardiac death, hypertension and other conditions closely related to alcohol abuse and its consequences.
But…. Russia failed to maintain this record, however: by 1987 the USSR was no longer able to enforce the anti-alcohol campaign and death rates rapidly resumed their upward trend from 1988 onwards. The anti-alcohol campaign was largely prohibitive and did not affect the attitude of the majority of Russia’s population towards alcohol. Thus towards the end of the Soviet period, the Russian population, faced with mortality rates much higher and life expectancy lower that than those of its western neighbors, was already confronting a health crisis which had been developing gradually over the previous two to three decades.
The period after 1991 • The health status of the Russian population declined precipitously following the collapse of the Soviet Union in late 1991. By all accounts, in the last decade Russia has been experiencing a shock unprecedented in peacetime to its health and demographic profiles.
Total mortality, 1990’s St. Petersburg Russian Federation
The leading causes of death in the Russia Federation • Cardiovascular diseases with rates that are the highest in the European Region (2005 – 56,4% (1, 3mlnfrom 2,3 died, or 905 cases per 100,000). • External causes of injury and poisoning (2005 - 13,7%). • Cancer (2005 - 12,4%).
CVD Injury Cancer
Causes of the mortality crisis • Major social and economic shock and income stratification in a population already vulnerable because of: • Poor diet, high levels of smoking, and weak systems of social support, in which alcohol and, increasingly, intravenous drugs, are easily available. • Health care system is poorly equipped to respond to challenges. • Furthermore new threats are emerging, in the form of infectious and parasitic diseases, including sexually transmitted diseases, and in particular AIDS, whose incidence has been growing exponentially since the latter half of the 1990s.
1997 “Concept of health care and medical science development in the Russian Federation”. Nominally, there are four main prioritiesemerging from this concept: • Health promotion, prevention and attention to lifestyles • Primary care development based on family practice • De-emphasizing secondary and tertiary care • Quality of care.
What ways we may use for improve Health in Russia? • Improve prevention • Reach everybody • Make it inexpensively
Role of FSU Internet PreventionNetwork in improvement Health in Russia • Networking Russian Public Health specialists via Internet • Improve prevention through the training of Russian Public Health specialists through Supercourse Library of lectures in Epidemiology, Public Health and Internet - www.pitt.edu/~super1/national/index.htm • Provide Russian Language Lectures on prevention via FSU Internet Prevention web site – www.pitt.edu/~super1/national/index.htm
FSUSupercourse Network, 2008 600registeredmembers
More than 250 lectures in Russian language www.pitt.edu/~super1/national/index.htm
FSU Supercourse 2008 Joint publications • Boyarsky S., Brener I., Vlasov V., Danishevski K., Dato V., Zabina H., Ivanov D., LaPorte R., Linkov F., Luchanski V., Troufanov A., Chepurnov A., Shubnikov E. Internet Prevention Program for Russia. Journal of Diseases Prevention and Health Promotion. Number 3, 2001, P.27-31.(in Russian) • R.Talshinsky et all. (Constructing a NATO Supercourse// Scientific Networking and the Global Health Network Supercourse. IOS Press, 2006. P.12-27. • E.Gursky, D.Zhuravlev, S.Koptilov, R.Laporte, A.Rossodivita, V.Chernakov, E.Shubnikov, A.Trufanov. Information Sharing Policy in Counteracting Chemical,Biological, Radiological and Nuclear Threats. Proc. International Conference on Emergencies, Moscow, April 18-20,2007. pp.356-367 (in Russian).
FSUSupercourse, 2008 All 15 Former Soviet Union Countries are involved Russian language web site - www.supercourse.pochta.ru More than 250 lectures in Russian language About 600 active members of the network 5 joint meetings during last 8 years Joint publications
Health Indicator • A Variable, susceptible to direct measurement, that reflects the state of health of person in a community. Examples include infant mortality rates, incidence rates based on notified cases of disease, disability days, etc. These measures may be used as components in the calculation of a Health Index. A Dictionary of Epidemiology / edited for the International Epidemiological Association by John M. Last; associate editors, Robert A.Spasoff…[et al.]. -4th ed. P.196.
Health Index • A numerical indicator of the health of a given population derived from a specified composite formula. The components of the formula may be INFANT MORTALITY RATES, INCIDENCE RATES, INCIDENCE RATE FOR PARTICULAR disease, or other Health Indicator. A Dictionary of Epidemiology / edited for the International Epidemiological Association by John M. Last; associate editors, Robert A.Spasoff…[et al.]. -4th ed. P.196.
Health Education • The process by which individuals and groups of people learn to behave in a manner conductive to the promotion, maintenance, or restoration of health. A Dictionary of Epidemiology / edited for the International Epidemiological Association by John M. Last; associate editors, Robert A.Spasoff…[et al.]. -4th ed. P.196.
Health • A State of complete physical, mental, and social well-being and not merely the absence of disease or infirmity (WHO,1948). • The extent to which an individual or a group is able to realize aspirations and satisfy needs, and to change or cope with the environment. Health is a resource for everyday life, not the objective of living; it is a positive concept, emphasizing social and personal resources as well as physical capabilities (WHO, 1984). • A State of equilibrium between humans and the physical, biological and social environment, compatible with full functional activity (J.Last, 1997). A Dictionary of Epidemiology / edited for the International Epidemiological Association by John M. Last; associate editors, Robert A.Spasoff…[et al.]. -4th ed. P.196.
Health Promotion • The process of enabling people to increase control over and improve their health. It involves the population as whole in the context of their everyday lives, rather than focusing on people at risk for specific diseases, and is directed toward action on determinants or causes of health. A Dictionary of Epidemiology / edited for the International Epidemiological Association by John M. Last; associate editors, Robert A.Spasoff…[et al.]. -4th ed. P.196.
There are many possibilities to find out the Country's Health Profilesfrom newspapers,books,TV,radio and of course Internet. • WHO data: http://www3.who.int/whosis/whsa/whsa_table1_process.cfm?path=whosis,whsa,whsa_table1,endpoint&language=english • World Bank Data http://www.worldbank.org/data/wdi2001/pdfs/tab2_19.pdf • Library of Congress Data http://lcweb2.loc.gov/frd/cs/rutoc.html
http://www.pitt.edu/~super1/lecture/ns0011/006.htm • Supercourse Team already created Health profiles Power Point presentations for all 15 Former Soviet Union countries based on Supercourse methodology of sharing best teaching materials between public health teachers worldwide.
http://www.pitt.edu/~super1/lecture/ns0011/006.htm • The idea is that we would have one person (speaking native language!)available in eachcountry to collect health indicator information. Both WHO and theWorld Bank have this information,but is not very user friendly, in that it is in tables, ours in PowerPoint slides.
We may use YouTube too! Health indices for FSU